Publication, Part of Health Survey for England
Health Survey for England, 2024
Official statistics, National statistics, Survey, Accredited official statistics
Social care for older adults
Summary
This report includes results from the 2024 Health Survey for England (HSE) describing the need for and receipt of social care among adults aged 65 and over. It compares social care needs and receipt by age, sex, household income, area deprivation, longstanding illnesses and health status.
Detailed tables accompanying this report can be accessed here.
Key findings
- 13% of adults aged 65 and over received help with at least one Activity of Daily Living (ADL) in the last month. This proportion was lower among men (11%) than among women (14%).
- 19% of adults aged 65 and over had received help in the last month with at least one Instrumental Activity of Daily Living (IADL). This proportion was higher among women (23%) than among men (14%).
- 66% of adults aged 65 and over did not need any help with ADLs and/or IADLs. This figure decreased with age, from 75% of those aged 65 to 69 to 49% of those aged 80 years and over.
- 24% of adults aged 65 and over had some unmet need for help with ADLs. This was more common among women (27%) than among men (21%).
- Prevalence of unmet need for help with IADLs was 16%. Similar proportions of men and women had some unmet need for help with IADLs (15% of men and 17% of women).
- Needing and/or receiving help with ADLs and/or IADLs and reporting some unmet need for help with one or more ADLs/IADLs was more common among those living in more deprived areas than among those living in less deprived areas.
- Those with a limiting longstanding illness were more likely than those with non-limiting longstanding illnesses or no longstanding illnesses to need and/or receive help with ADLs or IADLs, and to have unmet needs with help for ADLs/IADLs.
Introduction
Contents
The HSE has included questions on social care for adults aged 65 and over since 2011, with questions last asked in 2021. This report describes older adults’ need for social care and to what extent care is provided, including analysis by age, sex, income, area deprivation and longstanding illness.
The analysis is based on a representative sample of the adults aged 65 and over living in private households. Adults in hospitals and care homes were not included in the sample.
Background
Social care is the provision and receipt of help with personal care and domestic tasks to help enable individuals to live as independently as possible. It impacts the lives of many, including those who require formal care and support, their families, unpaid carers, and the social care workforce. Overall, social care affects over 10 million adults of all ages in England at any one time (Source: GOV.UK, 2021).
Between 2023 and 2024, local authorities in England spent £27.1 billion on adult social care. There were almost 2 million requests for adult social care support received by local authorities, 1.43 million of which was from older people. (Source: NHS England, 2024).
The UK's age structure is shifting towards older ages due to declining fertility rates and people living longer, resulting in a growing number of people of pensionable age relative to those of working age (Source: Office for National Statistics (ONS), 2022).
Methods and definitions
Methods
Questions for those in need of, or in receipt of, social care were asked of adults aged 65 and over.
The current modules of social care questions were developed in 2009 and 2010 and first used in the HSE 2011. They are designed to investigate different, but related, areas:
- the need for and receipt of social care among adults aged 65 and over
- how those services are provided by paid-for and unpaid carers
- the characteristics and experiences of adults who provide unpaid social care and support to family members, friends and neighbours
Core questions for adults aged 65 and over are included in HSE in every year. More detailed questions alternate every other year, covering either the nature of care received by older adults or focused on the experience of unpaid care givers.
More detailed information about the modules can be found in the HSE 2011 report.
Social care receipt was last reported on in 2021. Due to differences in survey methodology, direct comparisons with 2021 cannot be made. See the HSE 2021 Methods report for further information.
While social care may be needed by and provided for people of any age, the sample for the HSE does not include sufficient numbers of social care recipients among children and adults aged under 65 to allow robust analyses of the patterns of need and receipt of care among different groups. Therefore, these questions are only asked of adults aged 65 and over. Only private households were included in the sample, and older adults in hospitals and care homes are not covered.
The full questionnaires can be found within the HSE 2024 survey documentation, available on the first page.
Definitions
Measuring need for and receipt of social care: ADLs and IADLs
The need for and receipt of social care is measured using a number of Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs). ADLs are activities relating to personal care and mobility about the home that are fundamental to daily living. IADLs are activities which, while not fundamental to functioning, are important aspects of living independently. A total of thirteen ADLs and IADLs were used in the HSE and are shown in Table A; these were carefully selected to represent a full range of key activities.
The ADLs and IADLs included in the social care module allow an approximation of the Barthel Index, a measure of ability to live independently at home for older people. For further details see the 2011 report.
| ADLs | IADLs |
| Having a bath or shower | Doing routine housework or laundry |
| Using the toilet | Shopping for food |
| Getting up and down stairs | Getting out of the house |
| Getting around indoors | Doing paperwork or paying bills |
| Dressing or undressing | |
| Getting in and out of bed | |
| Washing face and hands | |
| Eating, including cutting up food | |
| Taking medicine |
Table B compares the national eligibility criteria with the ADLs and IADLs where there is an obvious correspondence.
| National eligibility criterion | ADL | IADL |
| Managing and maintaining nutrition. | Eating, including cutting up food. | Shopping for food. |
| Maintaining personal hygiene. | Having a bath or shower. Washing face and hands. |
|
| Managing toilet needs. | Using the toilet. | |
| Being appropriately clothed. | Dressing and undressing. | |
| Being able to make use of [their] home safely. | Getting up and down stairs. Getting around indoors. Getting in or out of bed. |
|
| Maintaining a habitable home environment. | Doing routine housework or laundry. | |
| Making use of necessary facilities or services in the local community, including public transport and recreational facilities or services. | Getting out of the house. |
There are no direct equivalents among the eligibility criteria for the ADL ‘taking medicine’ or the IADL ‘doing paperwork and paying bills’. Similarly, several of the national eligibility criteria – developing and maintaining family or other personal relationships; accessing and engaging in work, training, education or volunteering; and carrying out childcare responsibilities – have no equivalent ADLs or IADLs. Some of the ADLs and IADLs affect more than one criterion, for example being able to get in or out of bed, get up and down stairs and get around indoors all have an impact on most of those eligibility criteria concerned with daily home life, such as maintaining personal hygiene and managing toilet needs.
Although the HSE measures of need are not directly comparable with the 2014 Care Act eligibility measure, both sets of criteria identify adults with multiple needs for care and support, and there is likely to be some overlap between those needing help with two or more ADLs or IADLs and those qualifying under the national eligibility criteria.
Need for help and unmet need
For each ADL and IADL, participants aged 65 and over were asked whether they could:
- carry out the activity on their own
- manage on their own with difficulty
- only do the activity with help
- could not do it at all
Where ‘need’ for help is discussed in the report, it refers to people in the last three categories.
For the IADLs relating to shopping, housework and paperwork, participants were asked to exclude help which was provided simply because of the way household responsibilities were divided.
Participants who indicated that they needed some degree of help for at least one ADL or IADL were asked whether they had received any help in the last month.
‘Unmet need’ refers to cases where participants indicated that they needed help with a particular ADL or IADL but had not received any help with it in the last month. Participants could be receiving help with one or more activity but also have unmet needs for other ADLs or IADLs.
Care needs of adults aged 65 and over
Ability to perform ADLs and IADLs in the last month
Adults aged 65 and over were asked how well they could carry out each of the 13 Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs). Those who said they could only carry out the activity ‘with difficulty’, ‘only with help’, or could not carry out the activity at all were combined into a category of adults aged 65 and over who had need for help with that activity.
The ADLs that adults aged 65 and over were most likely to struggle with or need help with were getting up and down the stairs (23%), having a bath or shower (15%) and dressing or undressing (14%).
For most ADLs, participants who had some need for help were most likely to say that they could manage the activities on their own but with difficulty. A smaller proportion of adults aged 65 and over said that they could do these activities only with help, or not do them at all.
Among IADLs, adults aged 65 and over were most likely to need help with shopping for food (22%), doing routine housework or laundry (21%) and getting out of the house (18%).
For more information: Table 1
Need for help with ADLs and IADLs, by age and sex
66% of adults aged 65 and over reported not needing help with any ADLs or IADLs. As explained in the Introduction to this report, survey estimates are subject to a margin of error. It is likely that the proportion of adults aged 65 and over in the population who did not need help with any ADLs and/or IADLs was between 64.3% and 68.4%.
The proportion of adults not needing help decreased with age from 75% of those aged 65 to 69 to 49% of those aged 80 years and over. Conversely, the proportion of adults aged 65 and over needing help with one ADL and/or IADL increased with age, from 3% of those aged 65 to 69 to 11% of those aged 80 and over. Similarly, the proportion who needed help with two or more ADLs and/or IADLs was highest among those in the oldest age group, with 39% of those aged 80 and over needing help with two or more ADLs/IADLs. This compared with between 19% and 26% in younger age groups.
Among adults aged 65 and over, men were more likely than women not to need help with any ADLs/IADLs (70% of men and 63% of women). Conversely, women (29%) were more likely than men (23%) to need help with two or more ADLs/IADLs. The proportion of men and women needing help with one ADL/IADL were similar (6% of men and 8% of women).
Looking at specific activities, women were more likely than men to struggle or need help with the following ADLs and IADLs:
- getting up and down stairs (26% compared with 19%)
- having a bath or shower (16% compared with 13%)
- getting in and out of bed (12% compared with 9%)
- shopping for food (25% compared with 18%)
- doing routine housework or laundry (22% compared with 18%)
- getting out of the house (21% compared with 15%)
Conversely, men were more likely to struggle or need help with taking medicine (8% of men could do with difficulty/ only with help/ could not do compared with 6% of women).
For more information: Table 2 and Table A1
Receipt of help and unmet need in the last month, by age and sex
Help with ADLs
13% of adults aged 65 and over received help with at least one ADL in the last month. A higher proportion of women (14%) than men (11%) received help with at least one ADL in the last month.
The proportion of adults who received help with ADLs in the last month increased with age. It fluctuated between 10% and 12% among those aged 65 to 79 and was highest, at 18%, among those aged 80 and over.
Help with IADLs
19% of adults aged 65 and over had received help in the last month with at least one IADL. This was more common among women (23%) than men (14%).
The proportion of adults who received help with IADLs in the last month increased with age, from between 13% and 15% of those aged 65 to 74 to 30% of adults aged 80 and over.
Unmet need
Adults who had some need for help with an ADL or IADL but who had not received help with that activity in the last month were categorised as having unmet need. It was possible to have received help with one or more ADLs or IADLs and still have unmet need for help with others.
24% of adults aged 65 and over had some unmet need for help with ADLs in the last month. A higher proportion of women had some unmet need than men (27% of women compared with 21% of men).
Unmet need for help with ADLs increased with age, from 18% of those aged 65 to 69 to 37% of those aged 80 and over.
Prevalence of unmet need for help with IADLs in the last month was lower than for ADLs (16%, compared with 24% for ADLs). Similar proportions of men and women had some unmet need for help with IADLs (15% of men and 17% of women).
Unmet need for help with IADLs also increased with age, from 13% of those aged 65 to 69 to 24% of those aged 80 and over.
For more information: Table 3
Need for and receipt of help in the last month, by household income and sex
Data for this analysis is presented as age-standardised.
When controlling for age, those in higher income groups were less likely than those in lower income groups to need help with at least one ADL or IADL. In the lowest income group, 37% needed help with at least one ADL, and 36% needed help with at least one IADL. By comparison, these figures were 14% and 15% respectively among those in the highest income group.
A similar pattern was evident for receipt of help with ADLs or IADLs. The proportion who received help with ADLs or IADLs was highest among those in the lowest household income group (18% received help with ADLs and 24% with IADLs) and lowest among those in the highest income group (5% received help with ADLs and 9% with IADLs).
Prevalence of unmet need for ADLs and IADLs also varied by household income. For both ADLs and IADLs, those in the lowest income group were most likely to report some unmet need (31% had some unmet need for help with ADLs and 21% had unmet need for help with IADLs) while those in the highest income group were least likely to do so (12% had some unmet need for help with ADLs and 8% had unmet need for help with IADLs).
For more information: Table 4
Need for and receipt of help in the last month, by area deprivation and sex
Data for this analysis is presented as age-standardised.
When controlling for age, the proportion of adults aged 65 and over who needed help with ADLs and IADLs increased with level of area deprivation. For ADLs, the proportion increased from 19% in the least deprived areas to 50% in the most deprived areas. For IADLs, these figures were 19% and 52% respectively. These patterns were similar for men and women.
The proportion of adults aged 65 and over who received help with ADLs in the last month also varied by area deprivation, after controlling for age. The proportions receiving help for ADLs and IADLS increased from 9% for ADLs and 14% for IADLs in the least deprived areas to 25% for ADLs and 37% of IADLs in the most deprived areas. These patterns were similar for men and women.
Looking at the proportions of adults over 65 reporting some unmet need for help with ADLs and IADLs, these also increased with level of area deprivation when controlling for age. Similar patterns were observed for ADLs and IADLs, and for men and women. The proportion reporting some unmet need for help with ADLs increased from 16% in the least deprived areas to 40% in the most deprived; for IADLs the proportion with some unmet need increased from 11% in the least deprived areas to 30% in the most deprived.
For more information: Table 5
Need for and receipt of help in the last month, by longstanding illness
Longstanding illness is defined as ‘any physical or mental health condition or illness lasting or expected to last 12 months or more’. A longstanding illness is defined as limiting if the participant reports that it reduces their ability to carry out day-to-day activities.
55% of adults aged 65 and over who had a limiting longstanding illness needed help with ADLs. This compared with 8% with a non-limiting longstanding illness and 8% with no longstanding illness. A similar pattern was observed for IADLs where 54% of those with a limiting longstanding illness needed help compared with 7% of those with a non-limiting longstanding illness and 9% of those who did not have a longstanding illness.
Among those with a limiting longstanding illness, 27% received help with ADLs and 37% received help with IADLs in the last month. By comparison, among those with a non-limiting longstanding illness, 2% received help with ADLs and 5% with IADLs. Among those who did not have a longstanding illness, 3% received help with ADLs and 5% received help with IADLs.
Those with a limiting longstanding illness were also more likely than those with a non-limiting longstanding illness and those with no longstanding illness to report some unmet need for help with ADLs and IADLs. 46% of older adults with a limiting longstanding illness had some unmet need with help for ADLs in the last month, compared with 8% of those with a non-limiting longstanding illness and 7% of those who did not have a longstanding illness. A similar pattern was observed for IADLs: 30% of those with a limiting longstanding illness, 4% with a non-limiting longstanding illness and 6% with no longstanding illness reported some unmet need in the last month.
For more information: Table 6
Trends in need and receipt of help and unmet needs
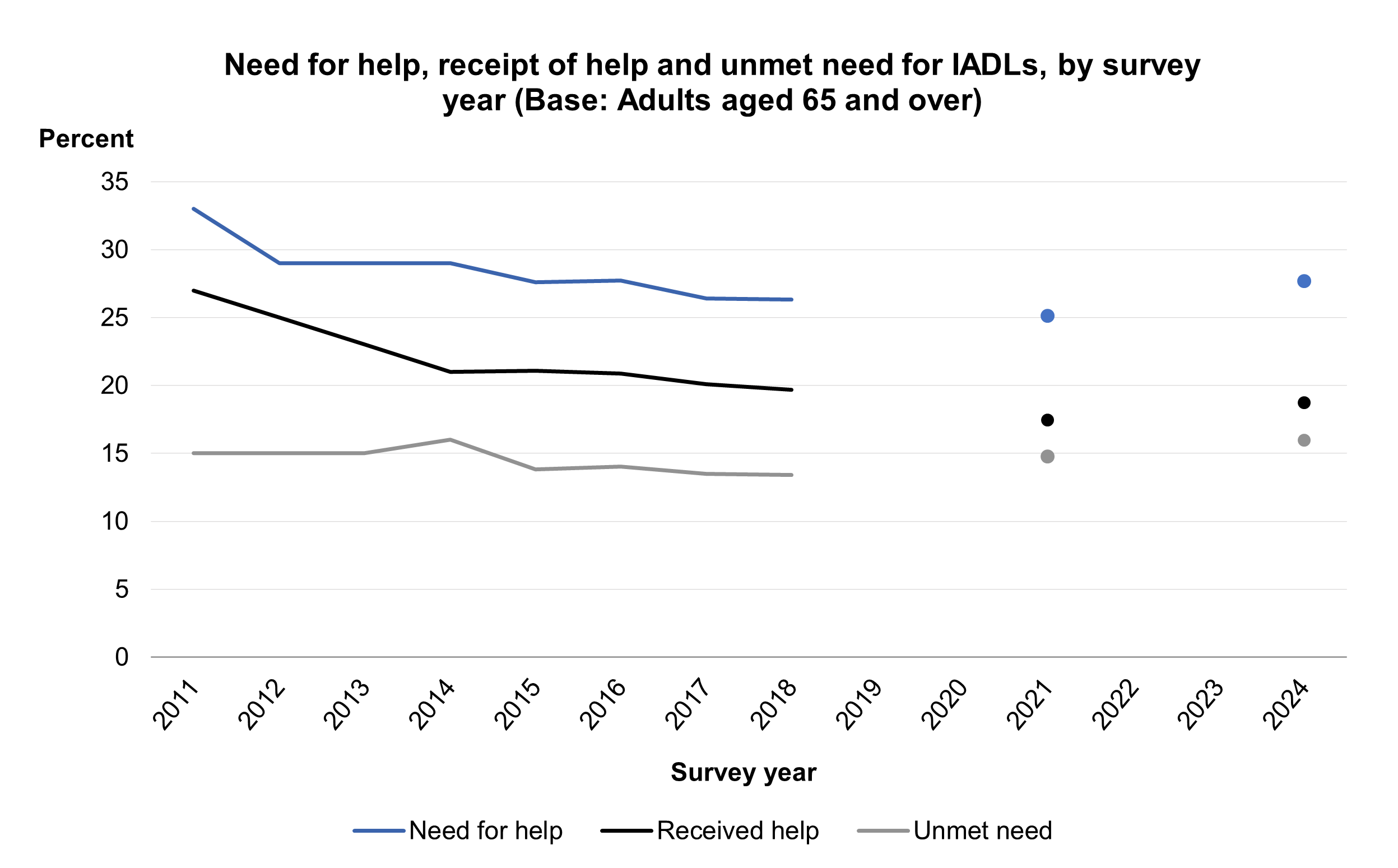
The levels of need for help, receipt of help and unmet needs were similar between 2018 and 2024. In 2024, 28% of adults aged 65 and over needed help with ADLs and 28% needed help with IADLs. In 2018, equivalent figures were at similar levels, at 27% and 26% respectively, having decreased from 32% (ADLs) and 33% (IADLs) in 2011. In 2024, 13% received help for ADLs and 19% received help for IADLs in the last month. Again, these figures were similar to those in 2018: 11% and 20%, and down from 15% (ADLs) and 27% (IADLs) in 2011.
The prevalence of unmet need for help with ADLs and IADLs remained relatively stable between 2011 and 2024. For ADLs, figures fluctuated between 26% in 2011 to 24% in 2018, with 2024 prevalence also at 24%. For IADLs, the proportion with unmet needs fluctuated between 15% in 2011 and 13% in 2018, with 2024 prevalence at 16%.
For more information: Table 7
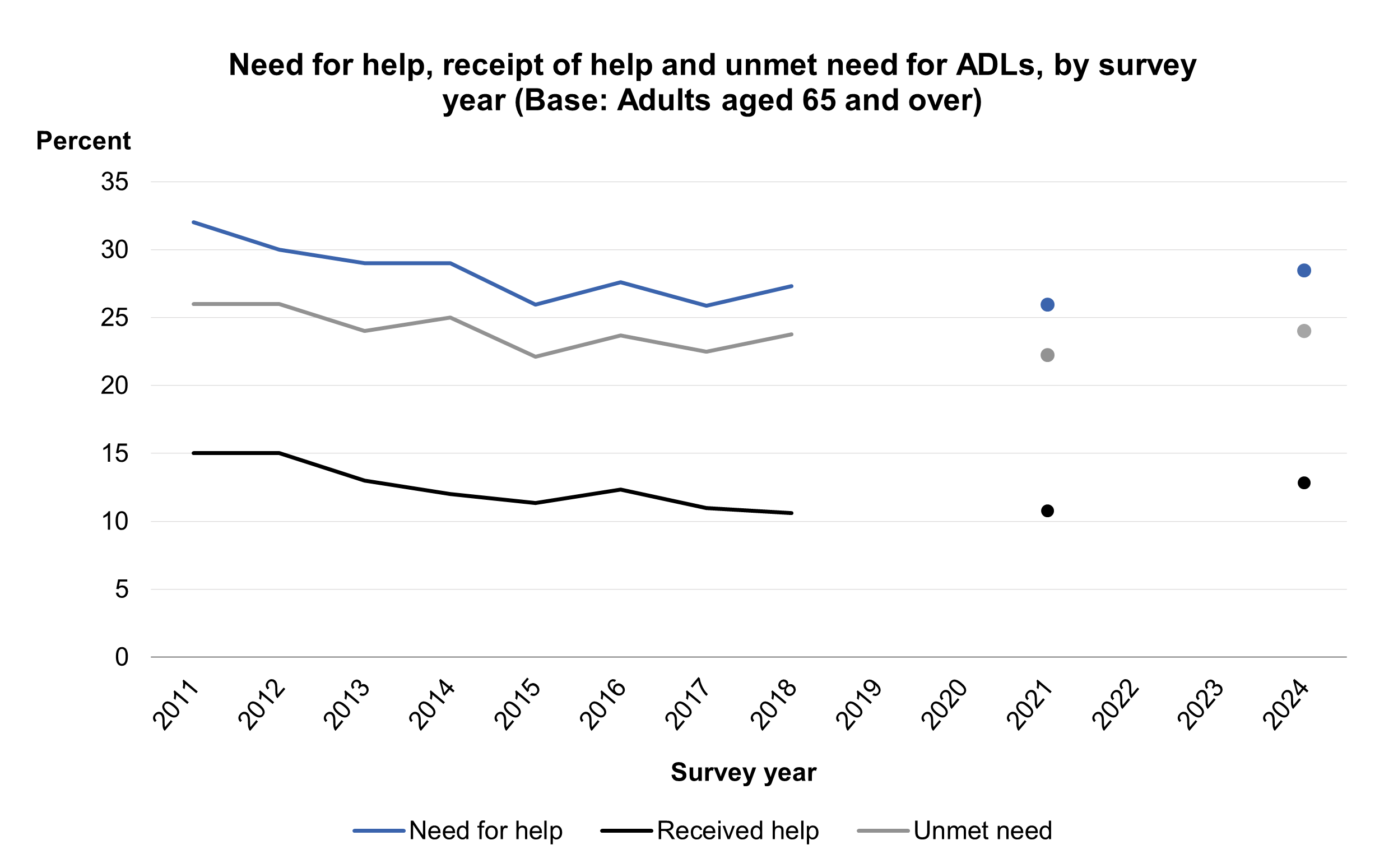
Note than 2021 data are not directly comparable with other years due to changes in survey methodology and response rates. See the HSE 2021 Methods report for further information.
Note than 2021 data are not directly comparable with other years due to changes in survey methodology and response rates. See the HSE 2021 Methods report for further information.
Last edited: 27 January 2026 9:34 am