Part of Data for Research and Development Programme - Evaluation
Appendix D: value for money
Highlights have been set out against the 4Es (economy, efficiency, effectiveness and equity) in the main body of the document. This appendix has been included to provide greater depth for those who wish to understand the basis of the findings.
In reviewing the Data for R&D programme for the value it has delivered against expectations, we will look at:
- the amount of funding received, how this compared to the original intent and how it has been spent
- the delivery against expected achievements set out in the Programme business case
- the progress against the original benefits set out
We have commented on the changes in context and challenges faced and made suggested recommendations throughout, both for the Programme as it progresses and to be taken into consideration in the future.
Funding and budget
The submitted programme business case (PBC) for the 3 years to 2024/25 sought investment of £200 million for the Programme. The original approval from the then Secretary of State (SoS) outlined a £25 million required reduction in funding from the NHS England allocation, granting £175 million. Through the initial duration of the Programme, further investments were secured from other sources, bringing the total investment for the 3 years to £206 million. As a result of the PBC Addendum submitted in 2025 and additional £81 million was granted for 2025/26 which brings the total to £290 million.
The funding breakdown table below shows the breakdown of the funding for the 3 completed years and the forecast for the current year. It should be noted that, as shown, approximately £20 million of the funding was on a pass-through basis for tangentially connected projects.
As can be seen in the spend profile table, there has been an average underspend of approximately £5 million per annum contributed to by a variety of factors, including delays in annual funding approvals and the split of capital and revenue. This funding has been split between central programme activities and support for the NHS England and regional SDEs.
* 25/26 – A transform budget has been created for this year only. This is a pot of money to be split amongst SDEs once they had submitted their business plans. Additional allocations over the baseline run and maintain allocations were based on these plans.
+ Across the Programme some funding has been provided on a pass-through basis which is not part of the core programme funding (that is, funding for Chair of Community of Practice). Some of this has been included in the 'Additional SDE Services' line but other sums have been wrapped into Portfolio lines. The totals by year for are shown in the bottom line of the table.
When looking at the way in which the money has been spent, we can comment on central Programme expenditure but not that of either the NHS England or regional SDEs. This is due to both the way in which the Programme operates, and also in how it is structured.
At a central level, the Programme complies with required commercial guidance on any procurement carried out directly, which is managed through the project management office (PMO) team (with the commercial team resources focussed on driving behavioural and procedural standardisation across the Network). Financial monitoring and reporting is carried out within the Programme for all central activities and projects with outline monitoring of wider spend.
The Programme has suffered significantly from ongoing uncertainty over annual funding and the fact that it has a limited lifespan. This has meant that resourcing on a permanent basis has been a continuing challenge and there are significant full-time equivalent (FTE) vacancies frequently in excess of 25%. In order to support activity, the Programme has been heavily reliant on both external and commissioning support unit (CSU) resourcing leading to a higher cost for resourcing than permanent FTEs. The basis on which the Programme has been funded makes this inevitable.
Whilst badged as a single programme it would be more accurate to describe there as being a central co-ordinating unit which runs the central activities and projects and which then commissions work and provides funding to SDEs, to deliver against agreed KPIs in the individual memorandums of understanding (MOUs). The regional SDEs are run by NHS trusts on their own or in conjunction with health innovation networks (HINs). The SDE architecture is hosted on trust platforms and, in many cases, will use staff from these parent bodies to deliver the services. While SDEs are required to provide annual bids outlining their plans for the year to secure specific funding, the funding provided does not cover the full cost and will be accounted for as a contribution towards the wider costs that support SDE delivery. This means that there is not a stand-alone reconciliation of how the funding provided through the SDE programme is spent available to the Programme.
The NHS England SDE, while being part of the central organisation, is at one remove from the Programme and is a commissioned service with a multi-year role. This remove, and the lack of common governance, means that the NHS England SDE does not have significant oversight from the Programme team and, despite being within NHS England, it shares with the regional SDEs the ownership of delivery rather than being a core part of the Programme.
The Programme leadership is aware of the weaknesses that exists in terms of the ability to track and manage spend more accurately and for 25/26 has introduced, or is in the process of introducing for next year, the following:
- For the current year it has introduced the concept of splitting funding bids into 'Baseline' and 'Transform' categories with Transform representing discrete projects to improve capability and capacity which can be more actively managed through the new account management function.
- As part of the planning for 2026/27 there is significant work being put into developing agreements which specifically increase the obligations on the SDE in terms of specific reporting on expenditure.
- Engagement has commenced to understand the necessary business systems including standardised customer relationship management (CRM) tool with linkages to finance systems and how this can be centrally provided and rolled out.
- The Programme is also commissioning work to develop a comprehensive performance management framework together with the supporting information required to monitor the proposed metrics.
Recommendation – The work on increasing transparency and accuracy of regional spend should be continued together with the ongoing discovery on the systems needed to automate the reporting of management information (MI), increasing transparency and reducing the reporting load.
Recommendation – As part of the work to support the previous recommendation, a clear direction needs to be set out on the basis of the need and purpose of all MI and how it will be used both to provide information to stakeholders and to provide insights which can help the SDEs to develop.
Recommendation - While the temptation to take a more command-and-control approach will be strong, HDRS should be mindful of the structure of the regional SDEs and the risks inherent in forcing specific behaviours, including the potential for them to walk away. At this time, we are not aware of increased statutory or legislative power to expressly mandate behaviours or actions, although it is expected that strong political support will be available.
Quantified benefits
It is not possible to assess the benefits delivered to date against the original case in a quantified way as the Programme does not currently have that information. The original PBC included a quantified benefits analysis for the preferred option, with a value of £1.7 billion over a 10-year period. With the reduction in funding, this was revised down to £1.4 billion and then, in January 2024, due to progress on the Programme, revised again, this time upwards to £1.6 billion, as shown below.
The work carried out to assess the potential benefits was detailed and took into account a number of factors when considering the value. This included:
- benefits adjusted down based on the application of a confidence grid, reflecting both the level of dependency and uncertainty regarding assumptions - this typically reduced benefit by 40-50%
- a maximum of 50% of the total benefit attributed to the investment - this reflected the additional role of other individuals and organisations, including researchers and individuals involved in implementation, in delivering benefits
The benefits in the case were backed up by an outline theory of change framework looking at inputs, throughputs, outcomes and impacts.
The Programme has struggled to measure metrics over time, due to the nature and attributed values of the individual benefits, the immaturity of the SDE Network and its data capture and reporting and some of the initial assumptions. As a result, a review was commissioned during 2025 and the finding a presented below.
Key findings and areas for improvement
Benefits statements captured within the financial year (FY) 2022-25 Programme Business Case and FY 2025-26 Programme Business Case Addendum ignore the fact that the Programme's role is primarily that of an enabler, limiting the ability to demonstrate measurable impact.
The most clearly attributable benefit is income generated from the SDE Network, which is currently captured in metrics however, this information requires validation and further detail is required from the SDEs to improve tracking of this benefit.
Additional benefits such as productivity gains, reduced duplication, improved processes, and regional standardisation have been discussed but remain undocumented.
Gaps in governance, standardisation, and supporting structures hinder consistent benefits management across the Programme.
Opportunities for improvement
- Strengthen governance and establish a dedicated benefits network.
- Standardise frameworks, templates, and reporting processes across the Programme.
- Redefine benefits statements to reflect measurable, attributable outcomes.
- Expand tracking to capture currently unrecorded benefits.
Following this piece of work a revised set of benefits and approach to capturing them has been developed and initial work to develop quantified value targets is underway with the initial outputs shown overleaf. Work on the revised framework being implemented is still underway and the values in the table (£20.177 million) are the current estimate for 2025/6, with it not being possible to determine values for earlier years at this time.
Benefits and approach to capturing them (.xlsx, 15.7KB)
While not disagreeing with the key findings of the internal review we believe that there is a need to consider a number of further factors in more detail.
The purpose of the Programme: The Programme was set up to create a collaborative ecosystem supporting research. At best it could be said to be building a foundation from which benefits could be delivered using existing structures at different levels of maturity and building on a 'brown field' site at a variety of pace. The creation of the Network is still at a relatively early stage despite the progress being made.
The role of the Programme: The Programme is intended to facilitate the ability to access high quality homogenous data from across care settings to support research across 6 primary use cases rather than to deliver end benefits itself.
The structure of the Programme: The central programme team has neither the mandate nor the leverage to make the SDEs behave in a structured way which, aligned with the varying maturity levels, means that the chances of successfully eliciting large amounts of complicated MI on benefits across the full system is limited.
Taken together, these exacerbate the underlying problems of the business case benefits basis.
Several of the benefits which were set out make assumptions, very possibly based on what were current areas of concern about where research would be focused. While cancer was and still is a significant concern the actual areas of research are significantly broader.
The case assumes that the Programme can influence, measure and deliver benefits when the Programme is in fact at one or more likely multiple removes from the delivery of the values, meaning that none of the listed benefits are direct benefits to the Programme. The only direct benefit so far seen would be income from providing the data and tools where it exceeds the direct cost of delivery, which was not included initially.
While attempts were made to reduce the level of the initial calculated values based on the linkage of empirical evidence to a causal chain as well as considering external factors it is not clear if the currency of the data, its specific relevance to the delivery of the benefit in the specific use case context, the quality of the data and the range and consistency if multiple sources existed were considered.
The timings of delivery for the benefits, in most cases, seem to be significantly faster than would normally be seen in a healthcare environment where changes in practice can take 6+ years to be adopted, and changes in treatment can take well in excess of 9 years to be tested and cleared. Whilst the benefits from clinical trials might be expected to deliver the soonest of those identified, including a quantified value in year 2 of a foundational programme seems excessive.
Additionally the case assumed that the existence of the programme would make things better in the chosen areas and deliver benefits when the findings from experience have suggested that in some areas such as DigiTrials the initial impact of the work has been to identify challenges which had not been previously known and highlighted weaknesses in data governance and access which need to be overcome before the undoubtedly significant benefits can flow.
Recommendation – Further work should be undertaken to reflect in the benefits targets the specific nature of the research work being undertaken across the various use cases. In other words, benefits should be linked to actual activities being supported rather than potential activities.
Recommendation – The Programme should consider the concept of whether a benefit is either:
- created (only exists because of what Data for R&D has done)
- enabled (Data for R&D has done something which allows another party to deliver a benefit)
- influenced (an activity contributes or steers a party at a remove or outside the public sector to deliver value)
This could be supported by more nuanced 'nested' Theory of Change assessment which considered the ownership of various stages of the journey to value delivery. The Programme can still measure its progress towards completing its part of the journey but cannot be held responsible for the success of subsequent stages.
Recommendation – We would caution against assuming significant levels of theoretically potential benefits which can be delivered at pace, when the first 3 years or so of activity will still predominantly be taken up with maturing the ecosystem, its data and its processes. This has been up to now, and will continue for some time to be, an investment for the future.
Qualitative achievements
The 5-case model structure for business cases uses a hierarchical flow but separates the elements out into the 5 cases. For the Programme these were:
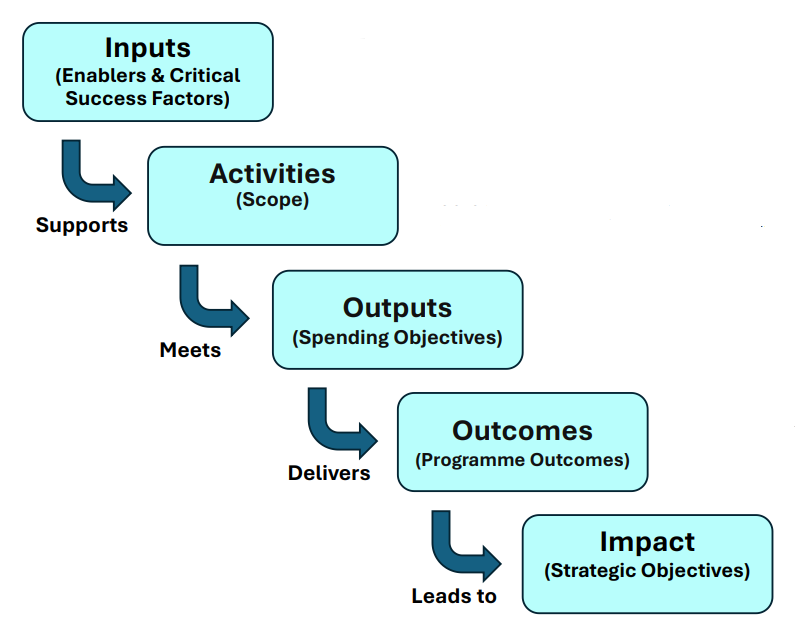
Inputs (enablers and critical success factors) - includes funding, NHS data assets, delivery partners, suppliers, programme team, patient and public involvement and engagement (PPIE) capability.
This supports:
Activities (scope) - deliver national and subnational TREs, federated datasets, clinical trial services, commercial framework, engagement and governance.
This meets:
Outputs (spending objectives) - delivered to time, cost and quality.
This delivers:
Outcomes (programme outcomes) - improved research capability, faster trials, efficiency gains, stronger life sciences sector public trust.
This leads to:
Impact (strategic objectives) - better health outcomes, sustainable NHS productivity, and UK global leadership in life sciences research.
Whilst the Programme was set up with a 3-year initial lifespan (although we are now over a year past that) the case was structured for a 10-year lifespan and therefore the more strategic elements (programme outcomes and strategic objectives) were set out for the medium and longer term.
When looking at what has been achieved at this point in time it is therefore more appropriate to look at the spending objectives, achievements to date and examples of where the SDE data is being incorporated into wider data analysis ecosystems with the potential to deliver value as well as understanding what still needs to be done.
These are the primary objectives that were intended to be directly funded and delivered by the Programme.
NHS-owned data infrastructure (strategic objective 1)
To develop an England-wide ecosystem of secure, NHS owned and managed data infrastructure providing access to high-quality, linked datasets. This will include a:
- national data platform expanded to support over 400 users
- network of 11 regional SDEs covering at least 80% of England
- national SDE
Achievements to date include:
- development of a national network of SDEs, all of which are operational
- establishing a national, scalable operating model for safe, sustainable, and trusted health data services, aligning with the NHS Long-Term Plan, Life Sciences Vision, and Sudlow Review
- development of a tested, interoperable approach (operational, commercial, technical and governance) which allows for projects to be conducted across multiple SDEs
- delivery of a 'single front door' through the HDR UK Gateway, where researchers can search for the data available, conduct cohort discovery and apply for multiple datasets through one process.
- launch of Research Powered by Data site, hosted within the NHS England website hierarchy, providing information on the SDE Network, case studies demonstrating the projects delivered, and information on service offering
- over 500 datasets available across the Network, the majority of which were not available or not easily available to researchers 3 years ago
- adoption of the Observational Medical Outcomes Partnership (OMOP) data model across the Network, meaning that data is able to be easily linked and grouped for analysis across multiple SDEs
- agreement to enable to single workspace per project for researchers, through a system of a 'lead SDE' which hosts all the data needed for a project
- over 500 projects completed or in progress across the SDEs, with more than 300 in pipeline
- developing a Health Data User Group and built-up membership to allow for close working with stakeholders to codesign and develop new services - comprehensive stakeholder engagement approach has seen positive testimonials from users
- securing increased collaboration with life sciences and industry partners, including AstraZeneca and Pfizer
- all but one of the SDEs have Section 251 approval - that is, a legal basis to process and provide access to identifiable data without consent
- consistent governance committees and processes to increase objectivity and standardisation applied across the Network
- securing £6.4 million in government funding for separate and complementary new data infrastructure projects to advance cancer research and AI model training
Increased clinical trials capacity and capability (strategic objective 2)
To use NHS data to improve trial setup, recruitment and delivery. This will include:
- 50% increase in trial recruitment by March 2025
- improved diversity of trial participants
- concierge support for high priority and innovative trials
Amongst our achievements to date, we have:
- enabled the design and delivery of large-scale clinical trials, inviting over 25 million citizens to participate in research studies, bolstering public engagement and trust
- supported recruitment of over 1 million volunteers for 5 major trials, including the world’s largest study (Our Future Health) and the UK’s fastest recruiting trial (Galleri)
- reduced feasibility insight generation timelines from months to hours through a feasibility tool with self-service opportunities
The expression of interest (EOI) in FY 2023/24 attracted interest from approximately 50 potential trials with the Recruitment Service selecting 8 for piloting. These are progressing at different speeds through the systems with the lessons learned to be summarised in Q1-2025. A further EOI will be launched before end FY 2024/25 with a longer time open to better attract industry studies and testing the model for other use cases (most will be smaller than the unusually large trials that NHS DigiTrials has serviced initially).
Behavioural science initiatives as embedded methodological research initiatives are being implemented to improve recipient decisions-making and to facilitate recruitment to trials from under-represented groups, supporting Our Future Health's national priority recruitment targets and helping ensure that trials are representative of the UK population.
Federated access to genomics datasets (strategic objective 3)
To enable interoperable and federated access to genomics datasets across multiple trusted research environments (TREs). This will include:
- a single point of access to datasets from UK Biobank, Genomics England, Our Future Health and others
- larger sample sizes and increased analytical power
Achievements to date include:
- advancing the Prostate Progress virtual registry, incorporating clinical and patient-entered data to improve prostate cancer care
- delivering the world’s largest genomics data research initiative, covering 6,000 cancer patients and integrating 75,000 radiology and 100,000 pathology images
Fair financial returns to the NHS (strategic objective 4)
To apply a coherent commercial framework to generate financial and non-financial returns. This will include:
- NHS share of UK clinical trial revenues exceeding 13% by March 2025
- demonstrable efficiency and cost avoidance benefits
Achievements to date include:
- delivery of an agreed pricing structure across the Network which recovers the costs of project delivery and derives additional value for the NHS determined by the future value of data usage
- progress in the development of a single contracting process to underpin the commercialisation of the service and increase speed of contracting
- establishing outline aggregated profit and loss monitoring for the ongoing monitoring of the Network and to support cross Network transparency
- break-even modelling completed identifying commercial requirements for achieving break even by end of annum 27/28
- bi-lateral and multi-party non-disclosure agreement (NDA) templates in place for use to support cross-SDE delivery
- early discovery work into investment opportunities for the Programme and for HDRS
- proposed approach to multi-SDE delivery models
- risk adjusted pipeline revenue for 25/26 forecast to be approximately £10 million (not all in year however)
Positive patient and public support (strategic objective 5)
To maintain and enhance public confidence in the use of NHS data for research and development, including:
- continuous patient and public involvement and engagement (PPIE) embedded at programme and project level
- measurement through engagement, feedback and research
Achievements to date:
Over 5,700 members of the public have been involved in PPIE work on health data over the past 3 years. This has been through a combination of large-scale public deliberations, work commissioned through understanding patient data and local PPIE work to support the development of regional SDEs.
Development of a community of practice, which brings together expertise from across the Network to solve problems and to work together on issues which affect the Network. The groups provide an additional delivery resource to the Programme and focus on technology and data, PPIE, IG and ethics, and communications.
Data use registers will be available across all SDEs by the end of the financial year, increasing transparency.
Summary of key points affecting value for money
Funding uncertainty and delays have had a material impact on the Programme's ability to deliver to original milestones.
Financial reporting is not strong or consistent enough to fully analyse wider spend but the Programme has stayed within its funding.
Efforts to improve data transparency, granularity, and objective-aligned reporting metrics should be sustained, alongside the implementation of automated systems.
Original benefits were inappropriate and overstated and, as they were for a 10-year programme, it is too early to assess in detail.
The original intent for collaborative benefits management has not worked in a loosely federated system with differing levels of maturity.
The Programme is still foundational at this point and is enabling rather than end-value delivery in nature. It should monitor its creation of capability, potential and opportunity rather than just specific outcomes.
The specific challenges in setting up and running the Network were over-simplified. Time and money has needed to be spent on further work to understand them. This is an ongoing process but critical for sustainability.
Material achievements have been made but the work to create a stable system with consistently high levels of maturity is still a work in progress with significant standardisation activity still to be completed.
The Programme structure as a federated network from which services are commissioned does not support easy direction and co-ordination. This will not be different in the future, and any new operating model will need to be designed with this in mind.
Last edited: 8 May 2026 11:51 am