Publication, Part of Adult Psychiatric Morbidity Survey: Survey of Mental Health and Wellbeing, England
Adult Psychiatric Morbidity Survey: Survey of Mental Health and Wellbeing, England, 2023/4
Accredited official statistics
Chapter 6: Drug use and dependence
Overview
Drug use, as addressed in this chapter, refers to the use of a substance for a purpose not consistent with legal or medical guidelines, for example the non-medical use of prescription medications or the recreational use of illicit drugs.
Participants were asked about lifetime and past year use of a range of illicit drugs including, for the first time in the survey series, the non-medical use of prescription opioids. Those who reported use of particular drugs in the past year were asked about signs of dependence on each drug used. The signs asked about were: daily use for two weeks or more, having a sense of need or dependence, inability to abstain, increased tolerance, and withdrawal symptoms.
This chapter draws on self-completion data to profile the prevalence and trends in illicit drug use and signs of dependence in the adult population of England.
Key findings
- Lifetime use of illicit drugs is common. One in three (33.0%) adults had used illicit drugs at some point in their life, with prevalence higher in men (38.9%) than women (27.5%). 3.1% of men and 3.2% of women reported having used an opioid medication (buprenorphine, fentanyl, morphine, oxycodone, or tramadol) that had not been prescribed to them.
- Illicit drug use in the past year was reported by one in nine adults (10.6%). This mostly comprised of cannabis, used in the past year by 11.4% of men and 6.1% of women. Past year use of any drug was highest in those aged 16 to 24 (18.1%) and 25 to 34 (19.2%).
- Signs of dependence on illicit drugs increased in prevalence from 3.8% of 16 to 64 year olds in 2014 to 6.7% in 2023/4. This rise mostly related to an increase in adults reporting signs of dependence on cannabis.
- Signs of dependence were more common in younger people and some ethnic groups. Among men, signs of drug dependence were most common in 25 to 34 year olds (14.2%). In women, they were most common in 16 to 24 year olds (9.4%). Prevalence was higher among adults in the Mixed/multiple/other ethnic group (7.8%) and lower among those identifying as Asian/Asian British (1.4%).
- Signs of dependence were associated with disadvantage, being more prevalent among adults struggling with debt (15.9%), those living in a more deprived area (7.3%), and those who were unemployed (12.9%) or economically inactive (9.9%).
- Signs of dependence were associated with poor mental health: 10.5% of adults with a common mental health condition reported signs of drug dependence, compared with 3.7% of those without a common mental health condition.
- A minority got support or treatment. One in five (21.2%) adults with signs of drug dependence had received support or treatment related to their drug use at some point in their life.
6.1 Introduction
Illicit drug use is common, but data sources on dependence are scarce. Estimates based on the 2024 Crime Survey for England and Wales (CSEW) indicate that one in twelve (8.8%) 16 to 59 year olds, and one in six (16.5%) 16 to 24 year olds, had used an illicit drug in the past 12 months (Office for National Statistics (ONS) 2024b). The CSEW found that the rate had been stable over time, with the same prevalence recorded in 2014 (8.8%). As a crime survey, however, the CSEW focuses on illegal activities, which can lead to underreporting. While it collects information on frequency of drug use, this is not a comprehensive indicator of drug dependence, and unlike APMS, the CSEW does not ask about other signs of dependence. While some people use drugs recreationally without long-term consequences, others develop dependence, which can lead to multiple health, social, and economic consequences.
Use and dependence on illicit drugs is associated with harms to health and premature mortality. In 2023, 5,448 deaths related to drug poisoning were registered in England and Wales, the highest number recorded since records began (ONS 2024a). Of these deaths, 3,618 were identified as drug misuse. There were also 9,690 hospital admissions for poisoning by drug misuse, with admissions almost five times more likely in the most - compared with the least - deprived areas. Hospital admissions for drug-related mental and behavioural disorders were also eight times more likely in the most, compared with the least deprived areas. They were also highest in ages 25 to 54, with this age group accounting for 70% of patients admitted for drug-related disorders (NHS England 2023). Substance use disorders have also been linked to poor health outcomes across a wide range of physical health conditions, with hospitalisation for substance use disorders associated with higher mortality rates and reduced life expectancy (Formánek et al. 2022).
Use and dependence on illicit drugs incurs high costs for society. The government estimated that illegal drugs cost society over £19 billion per year, with drug-related crime making up half of these costs (Black 2020). Data from the Home Office Homicide Index shows that between April 2018 and March 2023, there were 3,148 homicides recorded by the police, 1,627 of which were drug-related (52%) according to the current definition of drug-related homicide (ONS 2024c).
Drug dependence often forms a part of a profile of multiple adversity and disadvantage. In England, 336,000 people face at least three out of four of: substance use, homelessness, violence and abuse, and mental ill-health (Sosenko et al. 2020). A fifth of people starting substance use treatment had no home of their own in 2022/3, with the proportion highest among those starting treatment for opioid problems (Office for Health Improvement and Disparities (OHID) 2024).
Co-occurence of drug dependence and other mental health conditions is common but can cause challenges for treatment (Han et al. 2017; Delgadillo et al. 2013). Significant proportions of those treated as inpatients or in the community for severe mental illness also have problematic substance use (Phillips and Johnson 2003; Weaver et al. 2003). Likewise, over two-thirds of adults starting treatment for substance use said they had a mental health treatment need, an increase since 2018/19 (OHID 2024). The National Institute for Health and Care Excellence (NICE) guidelines for drug misuse prevention encompass targeted prevention efforts including educational programmes and family and community interventions (NICE 2017). The NICE guidelines are to be used in conjunction with DHSC’s Drug misuse and dependence: UK guidelines on clinical management (DHSC 2017), also known as the 'Orange Book', which provides advice to healthcare professionals on the delivery and implementation of a broad range of interventions for drug use dependence.
In 2021, Dame Carol Black’s independent review for drug treatment and recovery set out recommendations for increased focus on primary and early intervention and drug treatment and recovery, including reforms to policy, commissioning and practice (Black 2021). In the same year, the UK government launched a 10-year drug strategy From Harm to Hope, which proposed improvements to treatments for drug and alcohol use. This included enhancing the skills of the workforce in relation to drugs and alcohol treatments, reducing staff caseloads, provision of new drug and alcohol treatment places, integration of physical and mental health care with substance use services and improving access to treatment for adults experiencing multiple disadvantage (including combinations of homelessness, addiction, mental ill health, domestic abuse and contact with the criminal justice system) (HM Government 2021).
This chapter presents the prevalence of reported use of illicit drugs and signs of drug dependence in the adult general population and examines associations and the use of treatment and services. It is important to note that using a household survey to measure drug use and dependence will underestimate several key groups whose patterns and levels of drug use may be atypical. These include students in halls of residence, and those who are homeless or living in institutional settings (Chilman et al. 2024), including hospitals and prisons (Bebbington et al. 2021). Additionally, those experiencing drug dependence and living in private households may be less likely to participate in surveys, given that they may lead less stable lives or may be less able or willing to answer survey questions (Lader 2015). Hence household surveys are likely to underestimate the prevalence of drug dependence (Charles et al. 2021).
6.2 Definitions and assessments
Drug use and dependence
Drug misuse has been defined as the use of a substance for a purpose not consistent with legal or medical guidelines, for example the non-medical use of prescription medications or the recreational use of illicit drugs (ACMD 2008).
Drug use may impact negatively on people's lives leading to problematic drug use, and potentially to dependence. Dependence syndrome is defined in the International Classification of Diseases, 10th edition (ICD-10) as:
‘a cluster of behavioural, cognitive, and physiological phenomena that develop after repeated substance use and that typically include a strong desire to take the drug, difficulties in controlling its use, persistence in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal state.’ (WHO 1993)
Diagnostic criteria for dependent drug use are covered by the substance dependence codes F10 to F19 of the ICD-10, and are similar to the criteria specified in the fourth Diagnostic and Statistical Manual (DSM-IV; APA 1994). DSM-5 was launched in 2013 (APA 2013). The drug dependence questions used in the survey series were designed to DSM-IV criteria and have been used across the series to enable monitoring of trends over time.
A threshold of three or more of the following occurring together for at least one month, or occurring together repeatedly in the past 12 months is required for a diagnosis of substance dependence in ICD-10:
- Preoccupation with substance use
- Sense of need or dependence
- Impaired capacity to control substance-taking behaviour
- Increased tolerance
- Withdrawal symptoms, and
- Persistent substance use despite evidence of harm.
Measuring drug use and dependence
Questions about drug use were asked in the self-completion part of the interview, as in the 2000, 2007 and 2014 surveys (Roberts et al. 2016). They covered lifetime experience of over twenty types of named drug, together with use in the past year. Alongside the main drug name, a variety of informal terms were provided to help with recognition, for example ‘(marijuana, grass, hash, ganja, draw, skunk, weed, spliff)’ was listed in brackets after cannabis and ‘(laughing gas, whippets, nos, bulbs)’ was listed in brackets after nitrous oxide.
The drugs asked about are those considered to be mostly widely used and largely match those included on recent waves of the CSEW, with the addition of some further drug types such as volatile substances (described on the survey as ‘glues, solvents, gas or aerosols (to sniff)’) and amyl nitrite. Additional drugs were added to the questionnaire in 2023/4, such as khat, synthetic cannabinoids and non-medical use of prescription opioids, and were included in the summary use and dependence variables. As in 2014, new psychoactive substances (NPS) as a distinct category was not included, although some of the drugs asked about (such as mephedrone), could be classified as NPS.
For each of the following eleven types of drugs, further questions about signs of dependence were also asked:
- Amphetamines
- Cannabis
- Cocaine powder
- Crack cocaine
- Ecstasy
- Heroin or methadone
- Methamphetamine
- Non-medical use of prescription opioids (buprenorphine, fentanyl, morphine, oxycodone or tramadol)
- Synthetic cannabinoids
- Tranquillisers, and
- Volatile substances (glue, gas, aerosols or solvents).
Reported use in the past year was followed for these relevant drug types by five questions based on the Diagnostic Interview Schedule and designed to assess symptoms of drug dependence (Malgady et al. 1992). These questions asked about the past month and year, and covered:
- Daily use for two weeks or more
- Sense of need or dependence
- Inability to abstain
- Increased tolerance, and
- Withdrawal symptoms.
A positive response to any of the items was used as an indicator of possible drug dependence. This is a lower threshold than that recommended by ICD-10 and DSM-IV, and the set of questions does not include the diagnostic criteria of preoccupation and persistent use despite evidence of harm. However, the same approach and wording was used in the previous surveys in the APMS series and comparability has been maintained. Because people can be dependent on more than one type of drug, and because cannabis use accounts for such a large component of overall drug use, dependence was grouped into three categories, those:
- With no signs of dependence
- Who had one or more sign of dependence on cannabis only, and
- Who had one or more sign of dependence on another drug (including some who had signs of dependence on cannabis as well).
Measuring treatment
Participants who reported having ever used illicit drugs were asked whether they had ever received treatment and support services specifically related to drug dependence, including self-help advice or peer support, drug-related counselling or talking therapy, medication, detoxification or rehabilitation or other types of support.
In addition, all participants were asked about different types of mental health treatment and service use. These included current medication or psychological therapy for any mental or emotional problem, not necessarily for drug use or dependence, and a range of health, community and day care services over the past year.
6.3 Results
Prevalence of having ever used illicit drugs, by age and gender
A third (33.0%) of adults had used an illicit drug at some point in their life. Lifetime experience of drug use was associated with age and gender. Overall, 38.9% of men and 27.5% of women had taken an illicit drug at least once. Drug use was more likely to be reported by those aged 25 to 34 (46.3%) and 35 to 44 (44.2%), and less likely by those aged 75 and over (7.2%).
Men and women were more likely to have used cannabis than other drugs. Overall, 35.0% of men had used cannabis, 13.6% had used cocaine powder, 11.2% ecstasy, and 8.6% magic mushrooms (the next most commonly used drugs). Among women, 24.5% had used cannabis, followed by cocaine powder (7.2%), ecstasy (6.1%), and magic mushrooms (4.6%).
The age profile of users varied by type of drug. Those reporting that they had ever used amphetamines, amyl nitrite (poppers), heroin, khat, LSD, and methadone were more likely to be aged 45 to 54. While those reporting that they had ever used cocaine powder, ecstasy, ketamine, mephedrone, methamphetamine, nitrous oxide (laughing gas), and synthetic cannabinoids were more likely to be younger: aged 25 to 34.
Nitrous oxide (7.1%) was the third most cited drug taken by 16 to 24 year olds after cannabis (32.6%) and cocaine powder (7.7%), followed by ecstasy (6.6%) and ketamine (6.5%). While drug use has usually been found to be higher in men than women, this did not appear to be the case for all drug types among 16 to 24 year olds. For example, amyl nitrite (poppers) was reported by 4.1% of women and none of the men in this age group in the sample. Similarly, among 16 to 24 year olds, illicit use of tranquilisers was reported by 2.5% of women and 0.1% of men.
Introduced to the 2023/4 survey were new questions on whether participants had used any of a list of controlled prescription opioids that had not been prescribed to them. These were buprenorphine, fentanyl, morphine, oxycodone, and tramadol.
Overall, 3.2% of adults reported non-medical use of at least one of these types of prescription opioids. Men (3.1%) and women (3.2%) were equally likely to report having ever done this. Lifetime use was associated with age, being highest among 25 to 34 year olds (4.5%) and declining with age.
For more information: Table 6.1
Prevalence of illicit drug use in the past year, by age and gender
Overall, 10.6% of adults reported using an illicit drug in the past year. Drug use in the past year varied by age and gender. 13.8% of men and 7.5% of women had taken an illicit drug in the past year. Men aged 25 to 34 (26.9%) and women aged 16 to 24 (16.7%) were most likely to have taken any drug in the past year. For both men and women, the prevalence of drug use in the past year broadly declined with age.
Men and women were more likely to have used cannabis than other drugs in the past year. 11.4% of men had used cannabis, 3.6% cocaine powder, 2.1% ecstasy and 1.7% magic mushrooms (the next most commonly used drugs). Among women, 6.1% had used cannabis in the past year, followed by cocaine powder (1.2%) and ketamine (0.8%). Overall, 0.7% of adults reported misuse of prescription opioid medications in the past year.
After cannabis (17.9%), ketamine (4.3%), and ecstasy (4.1%), the types of drugs most likely to be used in the past year by 16 to 24 year olds were cocaine powder (3.8%), amyl nitrite (2.9%), and nitrous oxide (2.9%). The only participants to report past year use of volatile substances (such as glue) were women aged 16 to 24, 1.7% of whom reported this.
For more information: Table 6.2
Prevalence of illicit drug use in the past year, by ethnic group
Age-standardised prevalence of illicit drug use in the past year varied by ethnic group. Prevalence was highest among adults in the Mixed/multiple/other (15.2%) and White other (14.5%) groups and lowest among Asian/Asian British adults (3.1%).
For more information: Table 6.3
Prevalence of illicit drug use in the past year, by region
Prevalence of illicit drug use in the past year did not vary significantly by region.
For more information: Table 6.4
Prevalence of drug dependence, by age and gender
The prevalence of signs of drug dependence was measured for each of eleven types of drug:
- Amphetamines
- Cannabis
- Cocaine powder
- Crack cocaine
- Ecstasy
- Heroin or methadone
- Methamphetamine
- Non-medical use of prescription opioids that had not been prescribed to the participant (buprenorphine, fentanyl, morphine, oxycodone and tramadol)
- Synthetic cannabinoids
- Tranquillisers, and
- Volatile substances (glue, gas, aerosols or solvents).
For each drug, signs of dependence was defined as endorsing at least one of five questions about use of the drug (see Section 6.2). Dependent users were grouped into those who were dependent on cannabis only and those who were dependent on other drugs (including those who were also dependent on cannabis).
Overall, 5.4% of adults (95% CI 4.6, 6.3) showed signs of dependence on illicit drugs, which equates to approximately 2.5 million adults in England. This includes 4.3% (CI 3.6, 5.2) who showed signs of dependence on cannabis only and 1.1% (CI 0.8, 1.5) with signs of dependence on other drugs (with or without cannabis dependence as well).
Prevalence of dependence on any drug was higher in men (6.7%, CI 5.4, 8.4) than women (4.0%, CI 3.1, 5.0). Among men, signs of drug dependence were most likely in 25 to 34 year olds (14.2%, CI 9.5, 20.8), while in women, prevalence was highest among those aged 16 to 24 (9.4%, CI 5.4, 15.8).
For more information: Table 6.5 and Table A1 for confidence intervals
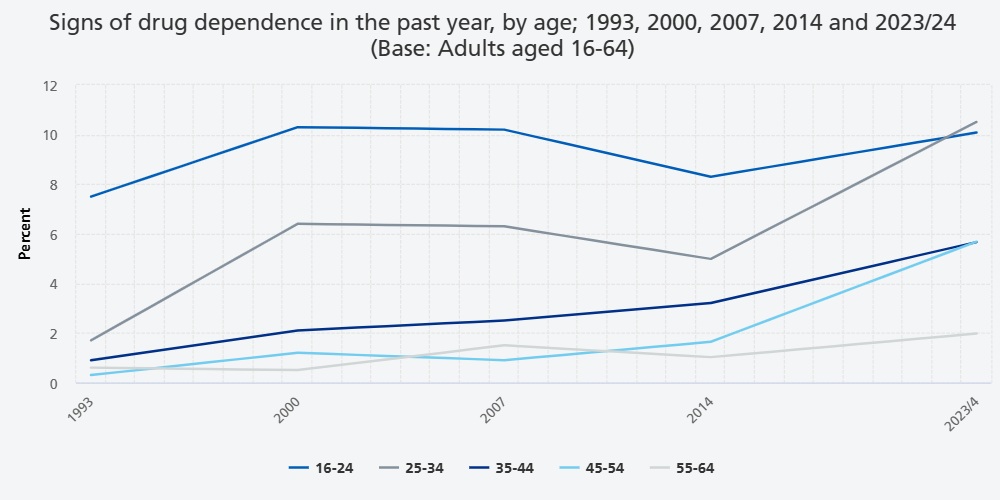
Signs of drug dependence in 1993, 2000, 2007, 2014, 2023/4
Note that the trend analyses were carried out by sex (male and female) rather than gender (men and women) to allow for comparison with 2014. See How to interpret the findings for information on how changes over time were assessed.
Between 2014 and 2023/4 signs of drug dependence increased in prevalence from 3.8% (95% CI 3.2, 4.5) to 6.7% (CI 5.7, 7.9), after a period of stability.
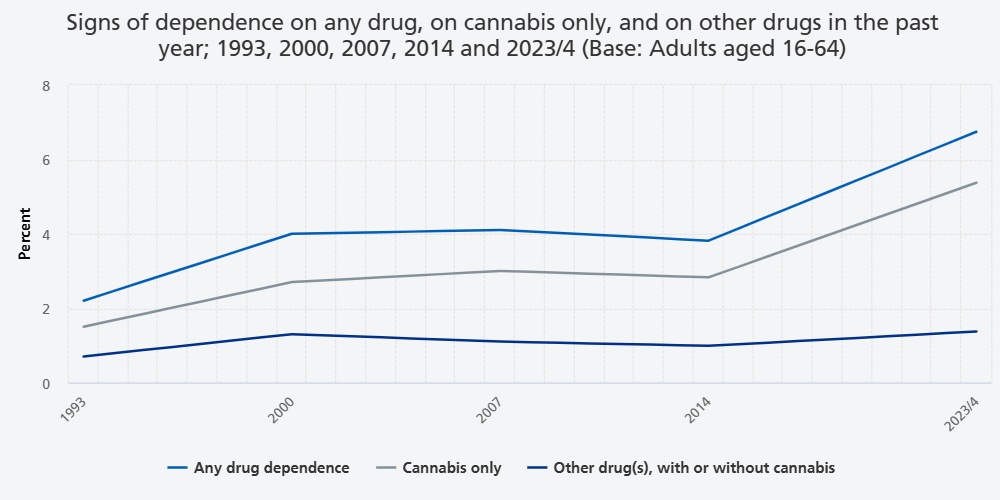
The increase in prevalence of signs of drug dependence was evident in both males (from 5.2% in 2014, CI 4.2, 6.5, to 8.3% in 2023/4, CI 6.6, 10.4) and females (from 2.4% in 2014, CI 1.9, 3.2 to 5.2% in 2023/4, CI 4.1, 6.5), and across most age groups. Signs of dependence related to cannabis use largely accounted for the upward trend, increasing from 2.8% (CI 2.3, 3.5) in 2014 to 5.4% (CI 4.4, 6.5) in 2023/4.
For more information: Table 6.6 and Table B1 for confidence intervals
Signs of drug dependence in the past year, by other characteristics
Ethnic group
Like the pattern observed for drug use, the prevalence of reported signs of drug dependence also varied between ethnic groups. In age-standardised analyses, the proportion reporting signs of dependence was highest among adults in the Mixed/multiple/other group (7.8%, 95% CI 4.0, 14.8) and lowest among adults in the Asian/Asian British group (1.4%, CI 0.5, 3.7). It should be noted that the confidence intervals for some estimates were wide and overlapping, so apparent differences between ethnic groups should be treated with caution.
For more information: Table 6.7 and Table A2 for confidence intervals
Employment status
The prevalence of reported signs of drug dependence varied by employment status. According to age-standardised analyses, 12.9% of working age adults (16 to 64) who were unemployed reported signs of drug dependence, compared with 9.9% of those who were economically inactive and 6.5% of those who were in employment.
For more information: Table 6.8
Problem debt
Problem debt was defined as being seriously behind with debt repayments or having utilities cut off. See the APMS 2023/4 Methods documentation for more information on how problem debt was derived.
In age-standardised analyses, the proportion of adults reporting signs of drug dependence was over three times higher among those with problem debt (15.9%) compared with those not experiencing problem debt (4.2%).
For more information: Table 6.9
Area-level deprivation
The proportion of adults reporting signs of drug dependence varied by area deprivation. Age-standardised prevalence was highest in the fourth (6.2%) and fifth (7.3%) most deprived quintiles.
For more information: Table 6.10
Region
The age-standardised prevalence of drug dependence in different English regions did not reach statistical significance.
For more information: Table 6.11
Comorbidity
Physical health conditions
In age-standardised analyses, adults with a limiting physical health condition were more likely to report signs of drug dependence (7.9%) than those without a limiting physical health condition (4.4%).
For more information: Table 6.12
Common mental health conditions
The age-standardised prevalence of drug dependence was 10.5% among adults with a common mental health condition, compared with 3.7% of those without a common mental health condition.
For more information: Table 6.12
Self-diagnosis and professional diagnosis of drug dependence
All participants were asked whether they had ever had any of a list of mental health conditions, including drug dependence. Participants who reported having experienced drug dependence were then asked whether they had ever been diagnosed as drug dependent by a professional, and whether they had experienced drug dependence in the past 12 months.
Overall, 2.2% of adults reported they thought they had been drug dependent at some point in their life and 0.7% reported that they had been professionally diagnosed with drug dependence. 0.4% of all adults had been diagnosed with drug dependence at some point and reported signs of drug dependence in the past 12 months.
Among those showing signs of drug dependence, one in four (24.9%) said they felt they had been drug dependent at some point in their life, compared with 1.0% of those with no signs of drug dependence. Men (28.8%) were more likely to self-diagnose drug dependence than women (16.4%).
6.3% of adults reporting signs of drug dependence had been professionally diagnosed at some point in their life. 4.1% of those reporting signs of drug dependence and who had been professionally diagnosed reported having had symptoms in the past 12 months.
For more information: Table 6.13
Treatment
Treatment and service use
Participants were asked about use of different types of mental health treatment and services. Two types of mental health treatment were asked about: current medication and psychological therapy for a mental or emotional problem. The use of a range of health, community and day care services over the past year were also asked about. This treatment and service use could have been for any mental health condition and was not necessarily related to drug use or drug dependence.
A third (33.4%) of adults reporting signs of drug dependence were receiving treatment for a mental or emotional problem, compared with 14.6% of those without signs of drug dependence. Adults reporting signs of drug dependence were more likely to be in receipt of medication (24.6%) than psychological therapy (12.9%), with 4.1% in receipt of both.
27.8% of those with drug dependence had used health care services for a mental or emotional problem in the past year, while 15.7% used community care services and 6.0% used day care services. Of those without drug dependence, 12.5% used health care services, 6.8% used community care services, and 3.7% used day care services.
For more information: Table 6.14
Psychotropic medication
Participants were asked which psychotropic medications, used to treat mental health conditions, they currently take (not necessarily relating to drug use and dependence). Overall, 12.5% of all adults were taking some form of psychotropic medication, with the most common medication types being those primarily used to treat depression (11.7%) and anxiety (10.7%). See Chapter 2 Mental health treatment and service use for more details.
A quarter (24.6%) of those reporting signs of drug dependence were taking psychotropic medication compared with 11.7% of those with no signs of drug dependence. The most common medications taken among adults reporting signs of drug dependence were those used to treat depression (22.4%) or anxiety (21.5%). 0.8% of those with signs of drug dependence were taking medication for substance dependence.
For more information: Table 6.15
Treatment and support specifically for drug dependence
Participants who reported having used illicit drugs in their lifetime were asked whether they had ever received treatment and support services specifically related to drug dependence, including self-help advice or peer support, drug-related counselling or talking therapy, medication, detoxification or rehabilitation or other types of support.
One in five (21.2%) adults reporting signs of drug dependence had received support or treatment related to their drug use at some point. Types of treatment and support used in relation to drug dependence included:
- Advice or information, including self-help or peer support such as Narcotics Anonymous (17.0%)
- Counselling or talking therapy (7.3%)
- Medication (4.3%)
- Detoxication or rehabilitation (2.7%)
- Other treatment or support (0.1%)
For more information: Table 6.16
6.4 Discussion
APMS is a key data source on drug use and dependence in England. While the annual Crime Survey for England and Wales (CSEW) provides key official statistics on trends in the prevalence of illicit drug use (ONS 2024b), APMS is also an essential resource in this field. Firstly, APMS data provide useful comparisons and a validity check on the CSEW drug use figures, and secondly because APMS includes questions related to drug use that are not available on the CSEW or elsewhere. These questions include: asking about types of drugs not currently included on the CSEW, questions that can identify people with signs of dependence on drugs, and data on comorbidities and use of treatment and services related to drug use.
Drug use may be more common than official statistics indicate. The results presented in this chapter suggest that a higher proportion of adults in England use drugs than official statistics from the CSEW might indicate. For example, while APMS found that 18.1% of 16 to 24 year olds used an illicit drug in the past 12 months, the CSEW figure for the same time period was 16.5% (ONS 2024b). Factors accounting for the difference might include variation in geographic coverage as the APMS sample did not include Wales. APMS also included drug types not covered on the CSEW, such as amyl nitrites, prescription opioids, synthetic cannabinoids, and volatile substances. However, even when comparing reported use of one drug type apparent differences seem evident: 4.3% of 16 to 24 year old participants on APMS reported use of ketamine in the past 12 months, compared with 2.9% of 16 to 24 year olds in CSEW. This suggests that relying on statistics based on reporting to a crime survey – which may experience greater social desirability bias in the disclosure of illegal behaviours – may lead to underestimating the true prevalence of drug use.
Monitor non-medical use of prescription opioids. There has been concern in other countries, in particular the United States, about non-medical use of prescription opioids (Hudgins et al. 2019). Until questions on this were added to the APMS 2023/4, relatively little was known about the extent to which prescription opioid medications were being used in England by people to whom they had not been prescribed. 3.2% of adults reported non-prescribed use of at least one of buprenorphine, fentanyl, morphine, oxycodone, and tramadol. The proportion is far higher than that for having ever used the opioid heroin (0.7%), indicating that use of non-prescribed opioids is currently distinct from that of heroin. The profile of those reporting such use is noteworthy for the lack of association with gender. That lifetime use was found to be highest among 25 to 34 year olds (4.5%) indicates that it’s unlikely to be explained by self-medication of medical disorders.
A changing gender profile. Among 25 to 34 year olds, men were twice as likely as women to report signs of drug dependence, which could in part reflect gender differences in age and nature of family formation responsibilities. However, in 16 to 24 year olds, rates of drug dependence were similar in men and women. In previous years of the APMS series, drug use and dependence were highest in 16 to 24 year old men. The apparent shift in profile of this youngest age group may indicate that men and women are becoming more similar to each other in these risk-taking behaviours. It is also possible that rather than convergence, drug use is starting at a later age in men and that subsequent problems with use may be developing in young men later than seen previously. Given the relatively small number of 16 to 24 year old participants in the sample, these patterns need to be examined further using other data sources.
The proportion of adults with signs of cannabis dependence nearly doubled this decade (from 2.8% in 2014 to 5.4% in 2023/4). This is despite no similar rise in the proportion of adults reporting past year cannabis use (7.2% in 2014, 8.7% in 2023/4). This upward trend might reflect known increases in cannabis potency. An analysis of drug seizures published in 2018 indicates the United Kingdom's cannabis street market has become increasingly populated by high-potency varieties of cannabis (Potter et al. 2018). A recent systematic review found more potent forms of cannabis were associated with greater likelihood of addiction (Petrilli et al. 2022). Innovation in terms of number and type of cannabis products and routes of administration available may have also led to increased availability and be associated with increased rates of dependence (e.g. cannabinoid vaping) (Freeman et al. 2015).
A minority of people with signs of drug dependence get drug-related support. The results presented in this chapter indicate that about one in five with signs of drug dependence had ever received support or treatment specifically related to their drug use. Furthermore, among people with a common mental health condition such as depression or an anxiety disorder, one in ten had signs of drug dependence. This may present challenges for mental health services in terms of engagement and recovery.
6.5 References
Advisory Council on the Misuse of Drugs (ACMD). (2008). Cannabis: Classification and public health. Home Office. https://www.gov.uk/government/publications/acmd-cannabis-classification-and-public-health-2008
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders, 4th Edition.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
Bebbington, P. E., McManus, S., Coid, J. W., Garside, R., & Brugha, T. (2021). The mental health of ex-prisoners: analysis of the 2014 English National Survey of Psychiatric Morbidity. Social Psychiatry and Psychiatric Epidemiology, 1-11.
Black, C. (2020). Review of drugs: Phase one report. Home Office. https://www.gov.uk/government/publications/review-of-drugs-phase-one-report
Black, C. (2021). Review of drugs: Phase two report. Department of Health and Social Care. https://www.gov.uk/government/publications/review-of-drugs-phase-two-report
Charles, H., Heron, J., Hickman, M., Brown, J., and Hines, L. (2021). Testing the validity of national drug surveys: comparison between a general population cohort and household surveys. Addiction, 116: 2076–2083.
Chilman, N., Schofield, P., McManus, S., Ronaldson, A., Stagg, A., & Das-Munshi, J. (2024). The public health significance of prior homelessness: findings on multimorbidity and mental health from a nationally representative survey. Epidemiology and Psychiatric Sciences, 33, e63.
Delgadillo, J., Godfrey, C., Gilbody, S., & Payne, S. (2013). Depression, anxiety and comorbid substance use: association patterns in outpatient addictions treatment. Mental Health and Substance Use, 6(1), 59-75.
Department of Health and Social Care. (2017). Drug misuse and dependence: UK guidelines on clinical management. https://www.gov.uk/government/publications/drug-misuse-and-dependence-uk-guidelines-on-clinical-management
Formánek, T., Krupchanka, D., Mladá, K., Winkler, P., & Jones, P. B. (2022). Mortality and life-years lost following subsequent physical comorbidity in people with pre-existing substance use disorders: a national registry-based retrospective cohort study of hospitalised individuals in Czechia. The Lancet Psychiatry, 9(12), 957-968.
Freeman, T. P., & Winstock, A. R. (2015). Examining the profile of high-potency cannabis and its association with severity of cannabis dependence. Psychological Medicine, 45(15), 3181-3189.
Han, B., Compton, W. M., Blanco, C., & Colpe, L. J. (2017). Prevalence, treatment, and unmet treatment needs of US adults with mental health and substance use disorders. Health Affairs, 36(10), 1739-1747.
Hudgins, J. D., Porter, J. J., Monuteaux, M. C., & Bourgeois, F. T. (2019). Prescription opioid use and misuse among adolescents and young adults in the United States: A national survey study. PLoS Medicine, 16(11), e1002922.
HM Government. (2021). From harm to hope: A 10-year drugs plan to cut crime and save lives. https://www.gov.uk/government/publications/from-harm-to-hope-a-10-year-drugs-plan-to-cut-crime-and-save-lives
Lader, D. (Ed.) (2015). Drug misuse: findings from the 2014/15 Crime Survey for England & Wales. Home Office. https://assets.publishing.service.gov.uk/media/5a7f1514e5274a2e8ab4a009/drug-misuse-1415.pdf
Malgady, R. G., Rogler, L. H., & Tryon, W. W. (1992). Issues of validity in the Diagnostic Interview Schedule. Journal of Psychiatric Research, 26(1), 59-67.
National Institute for Health and Care Excellence. (2017). Drug misuse prevention: targeted interventions. (NICE Guideline no. NG64). https://www.nice.org.uk/guidance/ng64
NHS England. (2024). Statistics on Public Health, England 2023. https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-public-health/2023
Office for Health Improvement and Disparities. (2024). Adult substance misuse treatment statistics 2023 to 2024: report. https://www.gov.uk/government/statistics/substance-misuse-treatment-for-adults-statistics-2023-to-2024/ adult-substance-misuse-treatment-statistics-2023-to-2024-report
Office for National Statistics (ONS). (2024a). Deaths related to drug poisoning in England and Wales: 2023 registrations. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/ bulletins/ deathsrelatedtodrugpoisoninginenglandandwales/2023registration
Office for National Statistics (ONS). (2024b). Drug misuse in England and Wales: year ending March 2024. https://www.ons.gov.uk/peoplepopulationandcommunity/crimeandjustice/articles/drugmisusein englandandwales/yearendingmarch2024
Office for National Statistics (ONS). (2024c). Measuring drug-related homicide methodology: February 2024. https://www.ons.gov.uk/peoplepopulationandcommunity/crimeandjustice/methodologies/measuring drugrelatedhomicidemethodologyfebruary2024
Petrilli, K., Ofori, S., Hines, L., Taylor, G., Adams, S., & Freeman, T. P. (2022). Association of cannabis potency with mental ill health and addiction: a systematic review. The Lancet Psychiatry, 9(9), 736-750.
Phillips, P., & Johnson, S. (2003). Drug and alcohol misuse among in-patients with psychotic illnesses in three inner-London psychiatric units. Psychiatric Bulletin, 27(6), 217-220.
Potter, D. J., Hammond, K., Tuffnell, S., Walker, C., & Di Forti, M. (2018). Potency of Δ9–tetrahydrocannabinol and other cannabinoids in cannabis in England in 2016: Implications for public health and pharmacology. Drug Testing and Analysis, 10(4), 628-635.
Roberts, C., Lepps, H., Strang, J., Singleton, N. (2016). ‘Chapter 11: Drug use and dependence’ in McManus S, Bebbington P, Jenkins R, Brugha T. (Eds) Mental health and wellbeing in England: Adult Psychiatric Morbidity Survey 2014. Leeds: NHS Digital.
Sosenko, F., Bramley, G., Johnsen, S. (2020). Gender Matters: Gendered patterns of severe and multiple disadvantage in England. Lankelly Chase.
Weaver, T., Madden, P., Charles, V., Stimson, G., Renton, A., Tyrer, P., ... & Ford, C. (2003). Comorbidity of substance misuse and mental illness in community mental health and substance misuse services. The British Journal of Psychiatry, 183(4), 304-313.
World Health Organization. (1993). The ICD-10 classification of mental and behavioural disorders. World Health Organization.
6.6 Citation
Maxineanu, I., Roop,S., Morris, S., McManus, S., Roberts, E., Strang, J. (2025) Drug use and dependence. In Morris, S., Hill, S., Brugha, T., McManus, S. (Eds.), Adult Psychiatric Morbidity Survey: Survey of Mental Health and Wellbeing, England, 2023/4. NHS England.
Last edited: 8 December 2025 3:02 pm