Data submissions from February 2025 onwards
Data submissions from February 2025 onwards are not directly comparable to previous months due to new submissions from independent providers that have resulted in an increase in the number of open referrals.
4 December 2025 13:00 PM
Introduction and Methodology
Introduction
Attention deficit hyperactivity disorder (ADHD) is defined by the World Health Organization as being characterised by a persistent pattern of inattention and/or hyperactivity-impulsivity that has a direct negative impact on academic, occupational, or social functioning, the level of which is outside the limits of normal variation expected for age and level of intellectual functioning.
The National Institute for Health and Care Excellence (NICE) currently estimate the global prevalence of ADHD in children to be around 5%, however this estimate is based on data published up to 2005. For adults in the UK NICE estimate the prevalence of ADHD to be around 3-4%.
A large representative cohort study (McKechnie, 2023) examining ADHD diagnoses and prescriptions in UK primary care between 2000 and 2018 reported that the overall rate of new ADHD diagnoses increased in this time. The rate doubled in males under 18; increased almost 20-fold in males over 18; quadrupled in females under 18 and increased 15-fold in females over 18.
This is believed to be the first analysis to consider the impact of the Covid-19 pandemic on ADHD diagnoses and medication prescribing in England.
Methodology
The analysis uses data held by the GP system supplier TPP. All data were linked, stored and analysed securely using the OpenSAFELY platform as part of the NHS England OpenSAFELY COVID-19 service. Data include pseudonymised data such as coded diagnoses, medications and physiological parameters. No free text data are included.
No GP data from patients who have registered a Type-1 Opt out with their GP surgery were included in this study.
All code is shared openly for review and re-use under MIT open license; https://github.com/opensafely/ADHD-Pre-and-Post-Covid. Detailed pseudonymised patient data is potentially re-identifiable and therefore not shared.
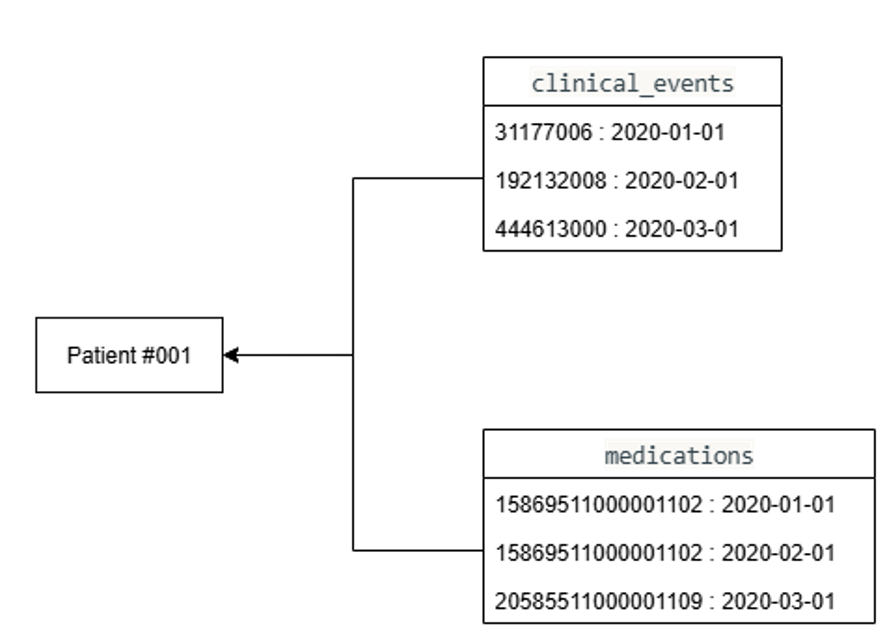
In all analysis undertaken only patients with a full GMS (General Medical Services) registration were considered. The TPP data schema for each patient is described in Figure 1. Each patient is linked with two tables; clinical events and medications containing a list SNOMED CT and dm+d codes respectively with dates of entry. A series of clinically verified SNOMED codes were used to identify an ADHD diagnosis and remission and d+md codes were used to identify licensed ADHD medication. A full list of codes is available in appendix 1, 2 and 3.
Diagnosis
Patients with an ADHD diagnosis code are selected alongside the date of the last logged diagnosis code. Patients with an ADHD remission code after the recorded ADHD diagnosis code are removed. Any patients that have died during the financial year are removed from the cohort.
ADHD medication prescribing
Prevalence of ADHD medication prescribing for patients with an ADHD diagnosis considers the first date of a recorded diagnosis code and the first date of a relevant medication code. If the medication code is before the diagnosis code the patient is rejected form the count.
Prevalence of ADHD medication for patients without an ADHD diagnosis considers the first date of a relevant medication code where the patient does not have an ADHD diagnosis code at any point in time. This analysis is used to identify how many patients may have been prescribed ADHD medication to treat another condition (e.g. narcolepsy).
ADHD medication prescribing in last six months
The percentage of patients with an ADHD diagnosis who have been prescribed ADHD medication in the last six months is calculated by computing two counts for each month interval form April 2016 to March 2025:
- Pdia - patients that have an ADHD diagnosis code in the given month (the ADHD diagnosis could have been given at any point in time).
- Pmed - patients that have an ADHD diagnosis code AND have been prescribed ADHD medication in the 6 months prior to the first day of interval month. This includes patients prescribed their first or subsequent ADHD medication.
The percentage of patients with ADHD who have been prescribed ADHD medication in the previous six months is defined by Pmed/Pdia for each month.
Time between ADHD diagnosis and medication prescribing
This is calculated by taking the difference between the date a patient was first prescribed ADHD medication and the date of their first diagnosis being recorded. To avoid counting patients with an ADHD diagnosis who are waiting to be assessed for ADHD medication, patients are counted in the year they were prescribed ADHD medication rather than the year they were diagnosed. Each patient is only counted once.
Other
All measures cover the period from April 2016 to March 2025.
Counts are rounded to the nearest 5. Data showing the time between ADHD diagnosis and medication is rounded to the nearest 10 and has patients aged 35 and over aggregated into a single group due to the presence of small numbers.
A patient is required to be registered in the financial year to be included in the analysis, thus the same patient can occupy multiple years. Patients must also be alive at the end of the financial year to be included in the cohort.
Patient age was defined from the date of birth to the start of the reporting year on 1st April.
Sex demographics only include males and females as recorded on the patient’s GP record.
Last edited: 4 December 2025 1:13 pm