Publication, Part of Breast Screening Programme
Breast Screening Programme, England, 2023-24
National statistics, Official statistics, Accredited official statistics
Main Report
Coverage is defined as the percentage of women in a population eligible1 for screening at a specific point in time who have had a test result recorded in the last three years.
Acceptable level is defined as attaining coverage levels of 70% or greater2.
Achievable level is defined as attaining coverage levels of 80% or greater2. All BSUs should be aiming for this standard.
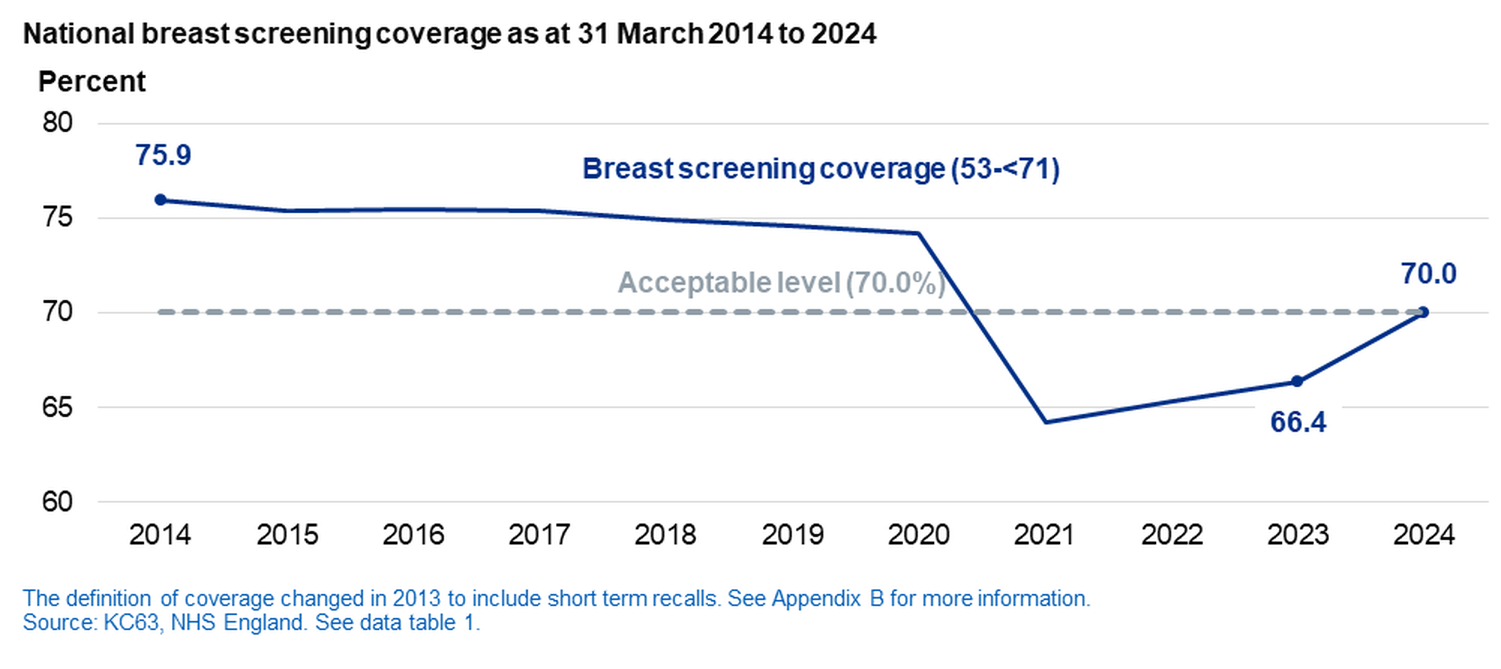
National coverage as at 31 March, 2014 to 2024
- In 2024, 6.59 million women were eligible for screening.
- Coverage was 70%, an increase of 3.6 percentage points from the previous year.
All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
National and regional (ages 53 to <71)
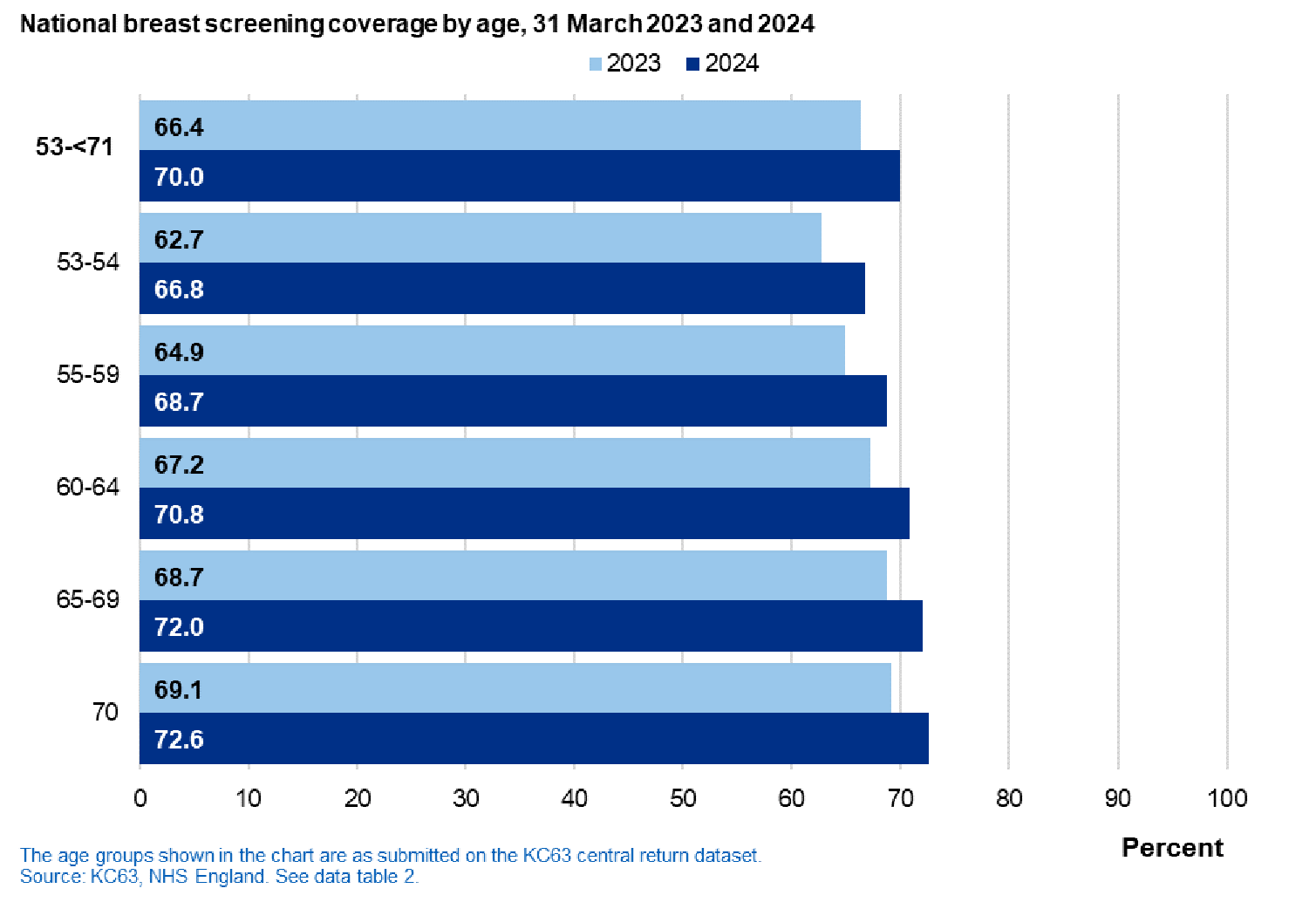
National coverage by age band, 31 March 2023 and 2024
- In 2024, coverage was highest amongst those in the 70 year age group and those aged 65-69 (72.6% and 72.0% respectively).
- Compared to 2023, coverage increased in 2024 for all age-groups within the 53 -< 71 age range.
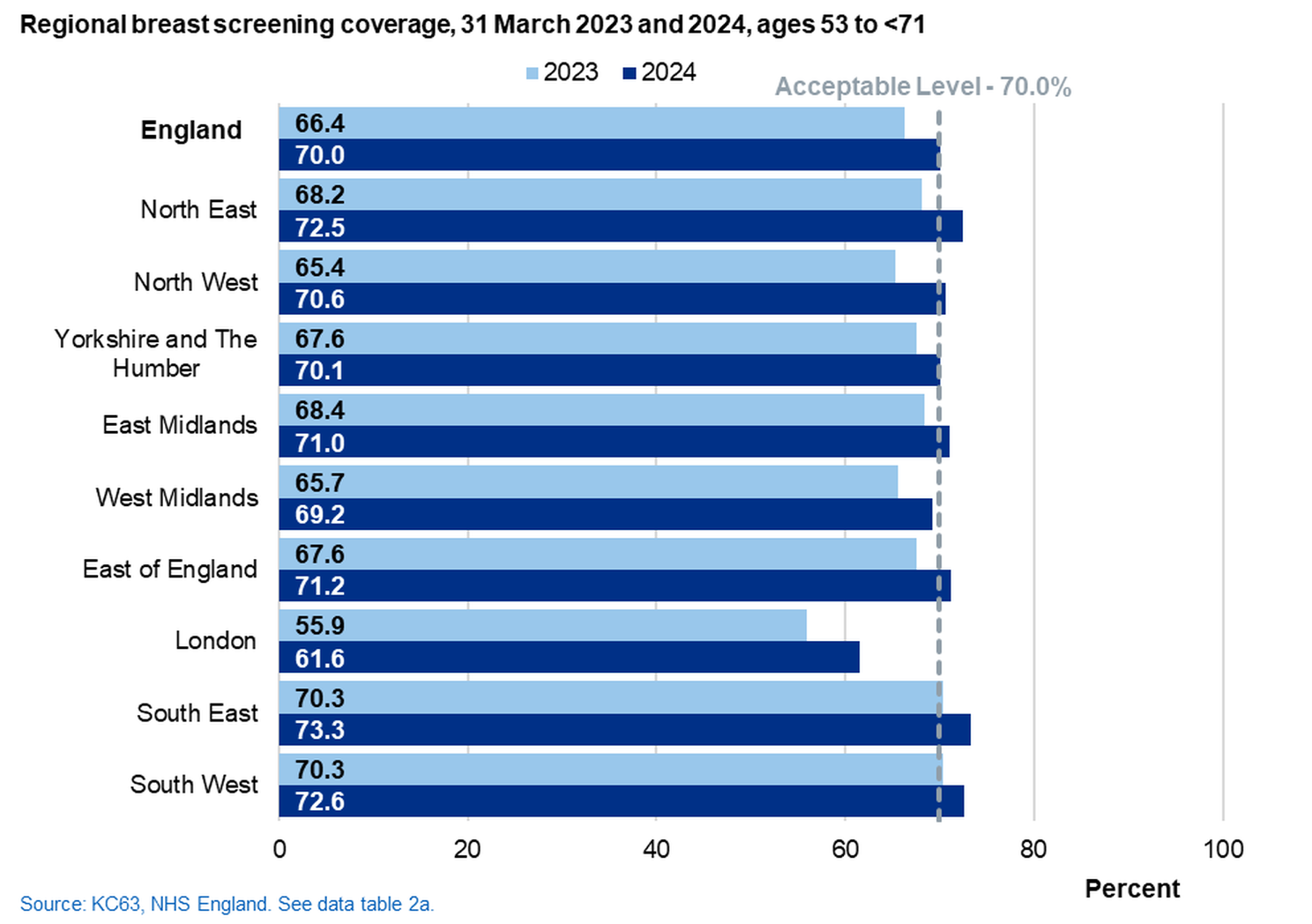
Regional coverage as at 31 March, 2023 and 2024
- In 2024, coverage increased in all regions. Coverage ranged from 61.6% in London to 73.3% in the South East.
Local authority (LA) (ages 53 to <71)

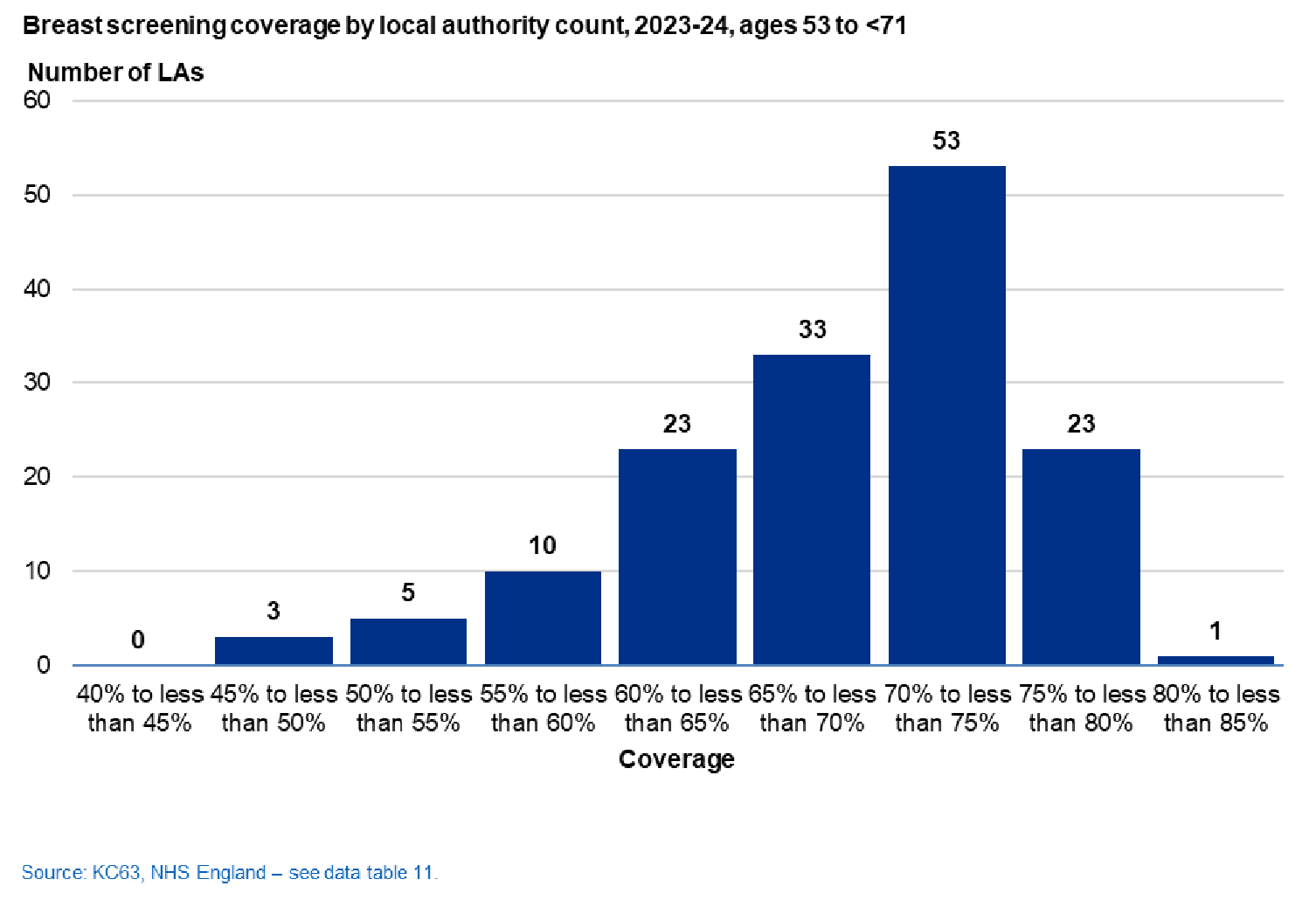
LA coverage as at 31 March 2024
- 77 of 151 LAs reached the acceptable level of 70% coverage, an increase of 34 compared to 2023.
- 1 LA reached the achievable threshold of 80%.
The Frequency chart below shows the number of LAs in each coverage category in 2023-24.
- The lowest coverage reported at LA level was 45.8% (Kensington and Chelsea), the highest was 80.8% (East Riding of Yorkshire).
- The full LA level data is available in table 11 of the data tables and the report dashboard.
Overall activity is measured for women aged 45 and over to include all screening activity; both those invited as part of the programme and those screened as a result of a self-referral.
- Since 2004, the programme screened women aged 50-<71 years.
- In 2009, the programme began to include a broader age range as part of the AgeX research trial, 47-49 years at the lower end and 71-73 at the upper end. Recruitment to the trial stopped in March 2020.
National activity, 2013-14 to 2023-24
- 1.95 million women aged 45 and over were screened within the programme in 2023-24, a decrease of 10.4% from 2022-23.
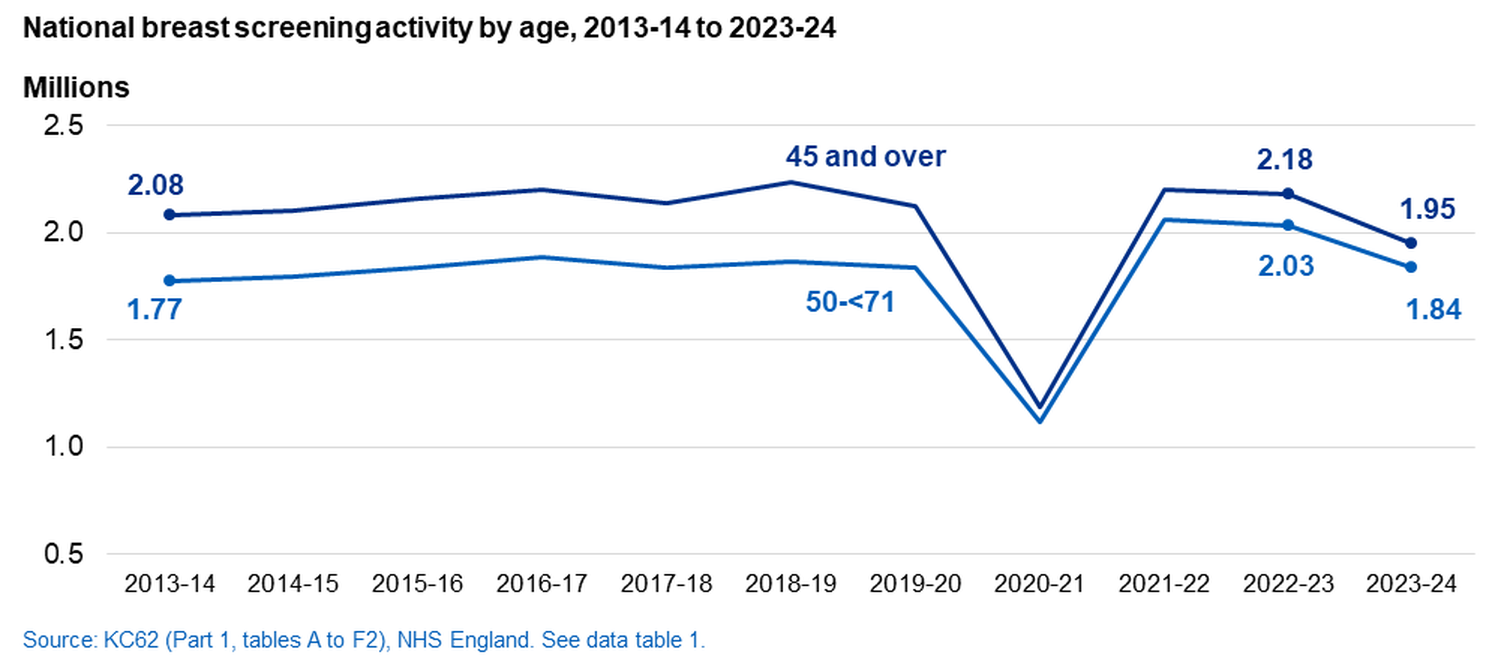
All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
National Screening Activity (ages 45 and over)
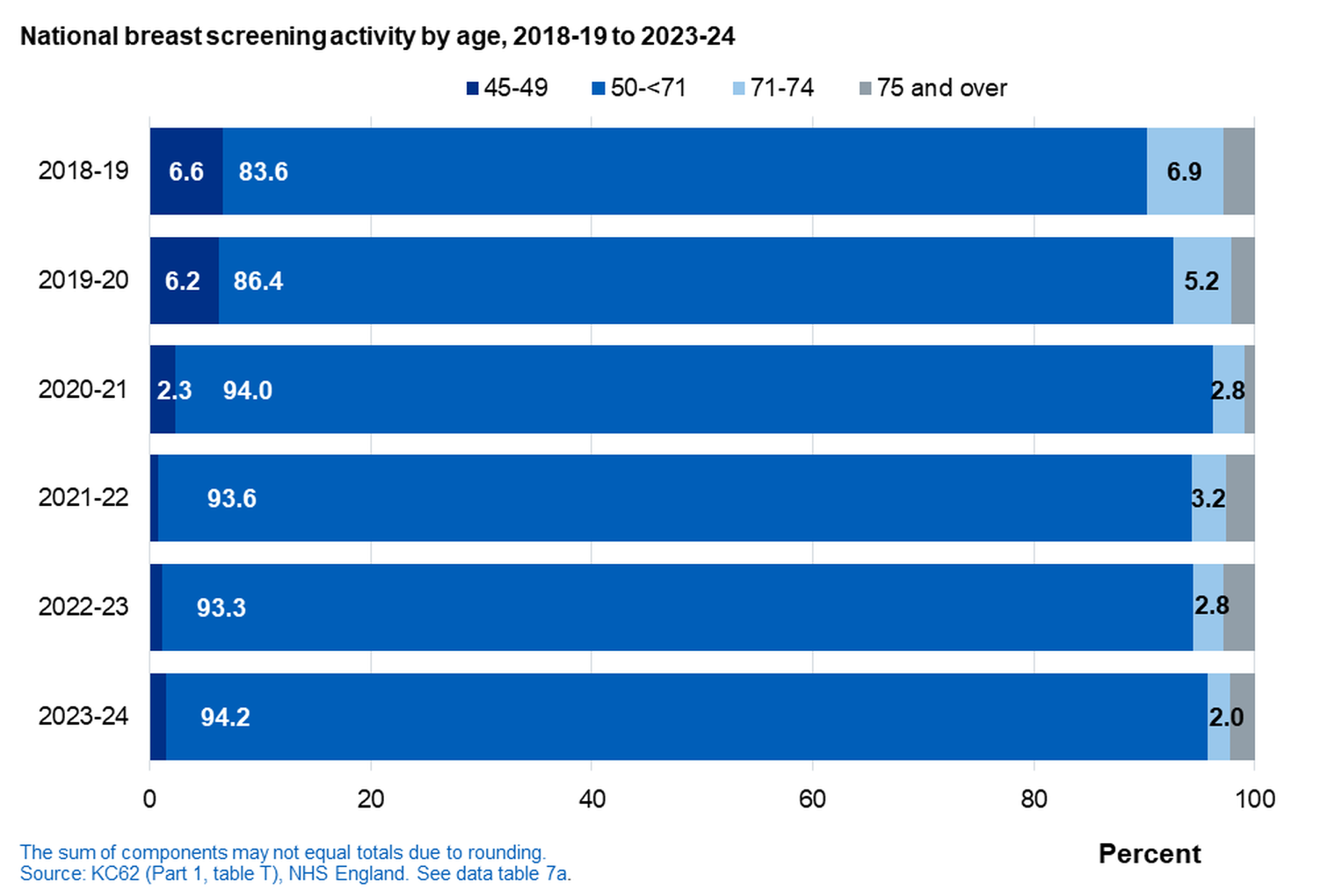
National activity, by age, 2018-19 to 2023-24
- In 2023-24, 94.2% of women screened were in the 50-<71 age category.
-
The Age-X trial recruitment ceased in March 2020.
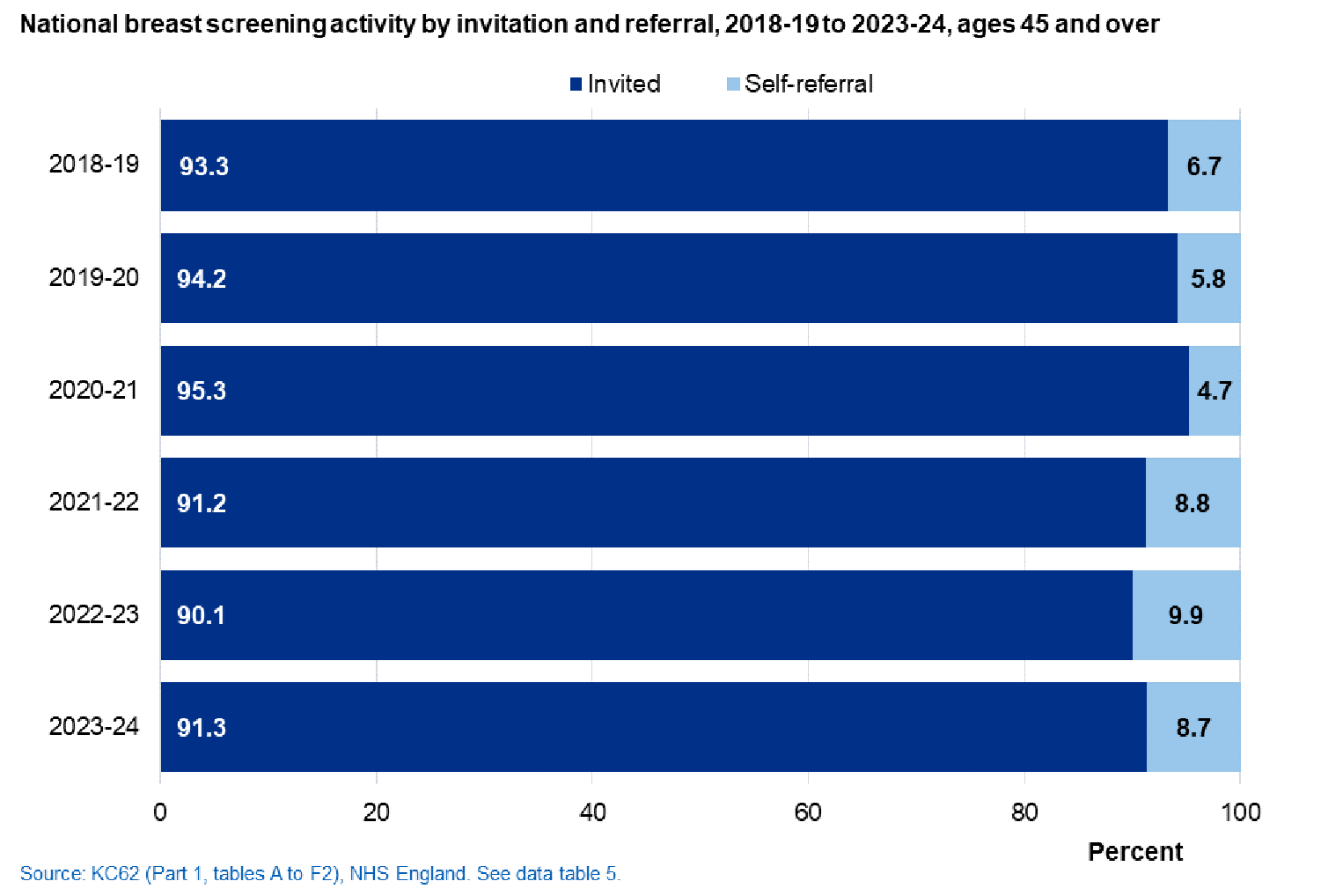
National activity, by invitation and referral, 2018-19 to 2023-24
- In 2023-24, 91.3% of women screened were invited as part of the programme; the remaining 8.7% were screened as a result of self-referral.
Self-referrals (ages 45 and over)
National activity for self-referral, by age, 2013-14 to 2023-24
The data collection definition is ‘self / GP referrals’, however, in all cases, it is expected that only self-referrals can be made. The report refers to 'self-referrals' rather than 'self / GP referrals'
- In 2023-24, 169,119 women were screened as a result of a self-referral, a decrease from 216,567 in 2022-23.
- 45.7% of self-referrals in 2023-24 were for women aged over 70 years.
- Between 2020-21 and 2022-23, there was an increase in the proportion of self-referrals in women of screening age (50<71 years). This has decreased in 2023-24.
- Women who self-refer are recorded in total screening activity, but are not included in invitation and uptake statistics due to their own request for screening. Consequently, the increase in self-referrals has a small negative impact on the rate of screening uptake nationally, as women aged 50<71 who self-refer and are screened are not included in national uptake statistics.
- Self-referrals are the most common point of entry to the screening programme for women aged 71 or over; these women are outside the target age group for invitation, but the programme does accept such referrals from this age group at three-yearly intervals. (See Appendix A).
- In 2020-21, there was a decrease in the number of self-referrals for all age groups. Contributory factors to this decrease include disruption from the COVID-19 pandemic, with services instructed to pause self-referrals for a number of months. See COVID impact summary for details.
Women are eligible to receive an invitation to be screened if they are in the screening age range (core 50 - <71), unless they are ceased due to having had bilateral mastectomies3 or individually opt out of screening4 or are ceased under a best interests decision.
The Age-X research trial, which invited women aged 47-49 and 71-73, ceased recruitment in March 2020.
National invites, 2022-23 and 2023-24
- In 2023-24, the number of women invited for screening was 2.55 million, a decrease of 16.1% from 2022-23 (45-74 years).
- There were 9,658 invitations in the 71-74 age group in 2023-24, a decrease of 35.5% from 2022-23.
The table below shows a breakdown of national invites by age for 2022-23 and 2023-24.
| Change from 2022-23 to 2023-24 |
|||||
| Age group | 2022-23 | 2023-24 | Number | % | |
| 45 and over | 3,038,312 | 2,548,823 | -489,489 | -16.1 | |
| 45-74 | 3,038,283 | 2,548,796 | -489,487 | -16.1 | |
| 45-49 | 40,489 | 43,658 | 3,169 | 7.8 | |
| 50-70 | 2,982,813 | 2,495,480 | -487,333 | -16.3 | |
| 71-74 | 14,981 | 9,658 | -5,323 | -35.5 | |
| Source: KC62 (Part 1, tables A to D) NHS England - see data table 4. | |||||
Invitations to screening
National, core programme (ages 50 to <71)
The programme categorises invitations into 5 groups, as summarised in the table (for further detail see Appendix C).
- In 2023-24, for women aged 50-<71 most invites (56.8%) were routine invitations to previous attenders where the last screen was within 5 years.
- The number of first invitations increased in 2023-24 by 4.6% from 2022-23.
- The majority of first invitations were to those in the 50-52 years age group, 305,716 in 2023-24 (up 10.2% from 277,401). See table 4 in data tables.
National invites, 2022-23 and 2023-24
The table below shows a breakdown of invitation type for 2022-23 and 2023-24 for those ages 50 to <71.
| 2022-23 | 2023-24 | ||||
| Type of invitation | Number (millions) |
% | Number (millions) |
% | |
| Total | 2.98 | 100.0 | 2.50 | 100.0 | |
| First invitation for routine screening | 0.34 | 11.3 | 0.35 | 14.1 | |
| Routine invitation to previous non-attenders | 0.39 | 13.1 | 0.35 | 14.0 | |
| Routine invitation to previous attenders (last screen within 5 years) |
1.91 | 64.0 | 1.42 | 56.8 | |
| Routine invitation to previous attenders (last screen more than 5 years) |
0.35 | 11.6 | 0.38 | 15.1 | |
| Short term recall | 0.00 | 0.0 | 0.00 | 0.0 | |
The sum of components may not equal totals due to rounding.
Source: KC62 (Part 1, tables A to D) NHS England – see data table 4.
Uptake is the proportion of eligible women who have a technically adequate screen ≤6 months of date of first offered appointment (see Appendix B).
Acceptable level is defined as attaining uptake levels of 70% or greater2.
Achievable level is defined as attaining uptake levels of 80% or greater2. All BSUs should be aiming for this standard.
One of the objectives of the screening programme is to maximise the number of eligible women who attend for screening. This is set out in the NHS Breast Screening Programme screening standards2. The performance levels provide a way to monitor progress.
Where ‘routine invitation’ is used this indicates that short term recall invitations5 are not included. Measurement of the national standard excludes short term recall invitations and self-referrals.
In September 2020, in response to COVID-19, open invitations were recommended rather than timed invitations to maximise utilisation of screening slots. This may have impacted uptake of invitations. See COVID impact summary for more details.
Uptake* of invitations
National and regional (ages 50 to <71)
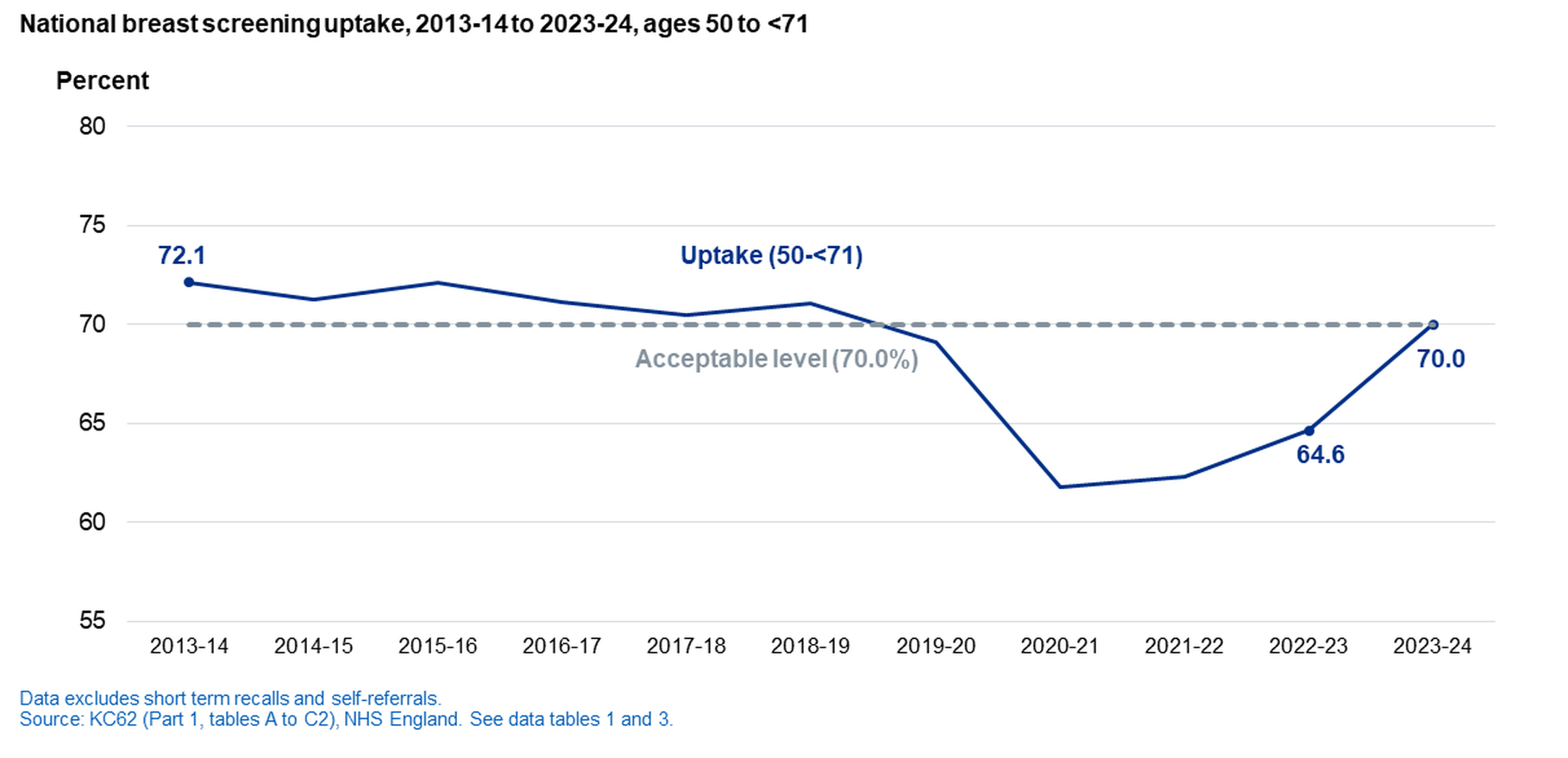
National uptake, 2013-14 to 2023-24
- In 2023-24, 1.75 million women who received an invitation** were screened by the programme. Down from 1.93 million in 2022-23.
- Uptake of invitations** increased to 70% in 2023-24, up from 64.6% in 2022-23.
Regional uptake, 2022-23 and 2023-24
- Uptake by women aged 50-<71 increased in all regions in 2023-24.
- Uptake ranged from 62.8% (London) to 72.9% (South East).
*All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
** Invitation figure used to calculate uptake includes first and all routine invitations. This does not include short term recalls.
By invitation type
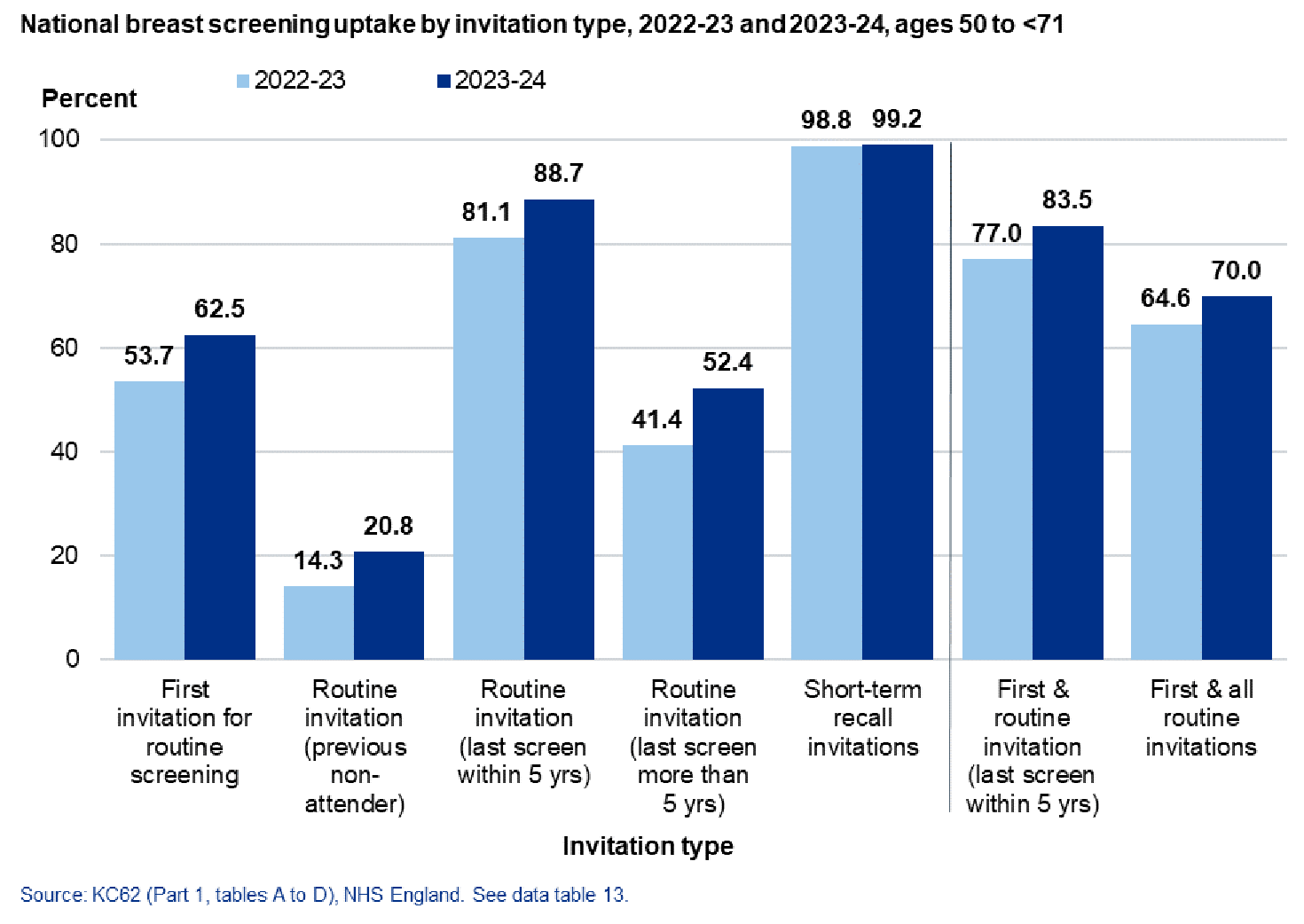
National uptake, 2022-23 and 2023-24, by invitation type, ages 50-<71
- 62.5% of women receiving their first invitation in 2023-24 were adequately screened.
- Uptake was lowest (20.8%) amongst women who received a routine invitation, having failed to respond to a previous invitation(s).
- Uptake was highest (99.2%) amongst those receiving short term recall invitations.
- Uptake has increased in every invitation type in 2023-24 when compared to 2022-23
National uptake, 2013-14 and 2023-24, by invitation type
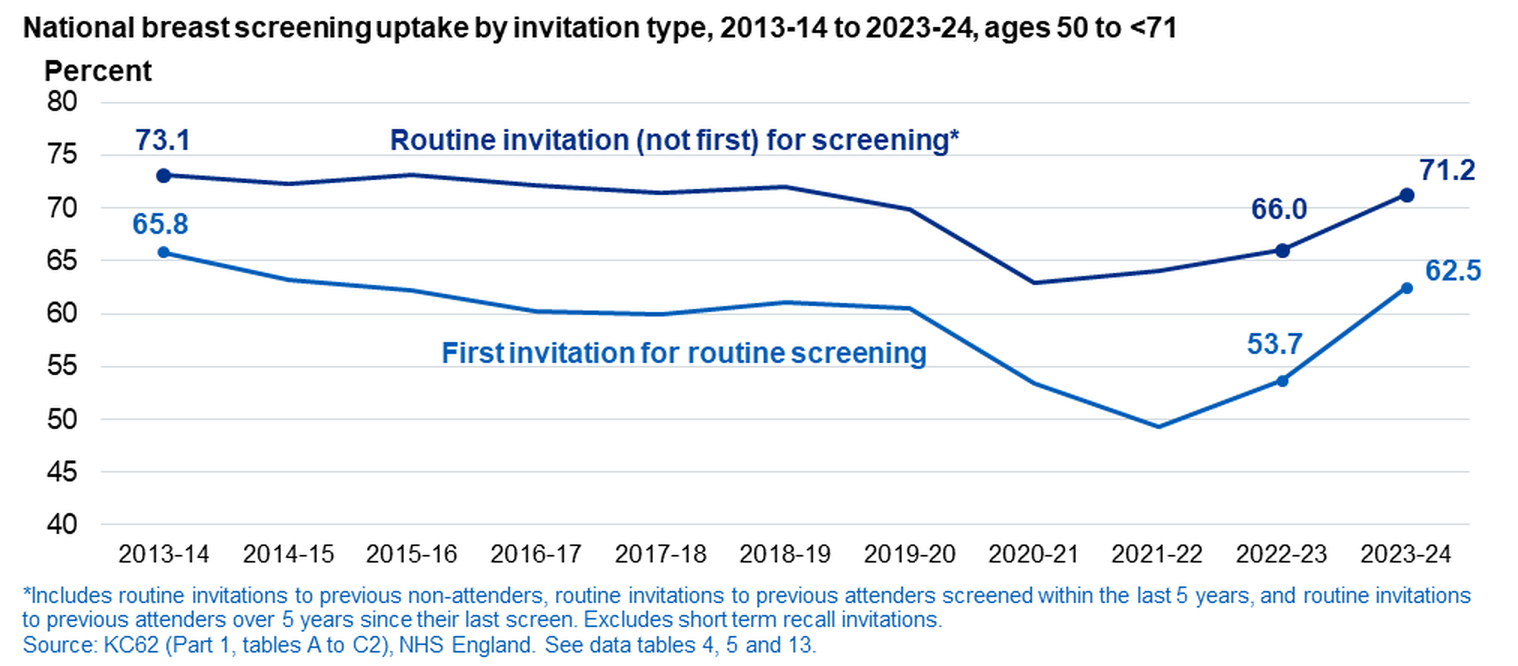
All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
Breast screening unit (BSU) (ages 50 to <71)
National uptake, 2022-23 and 2023-24, by BSU
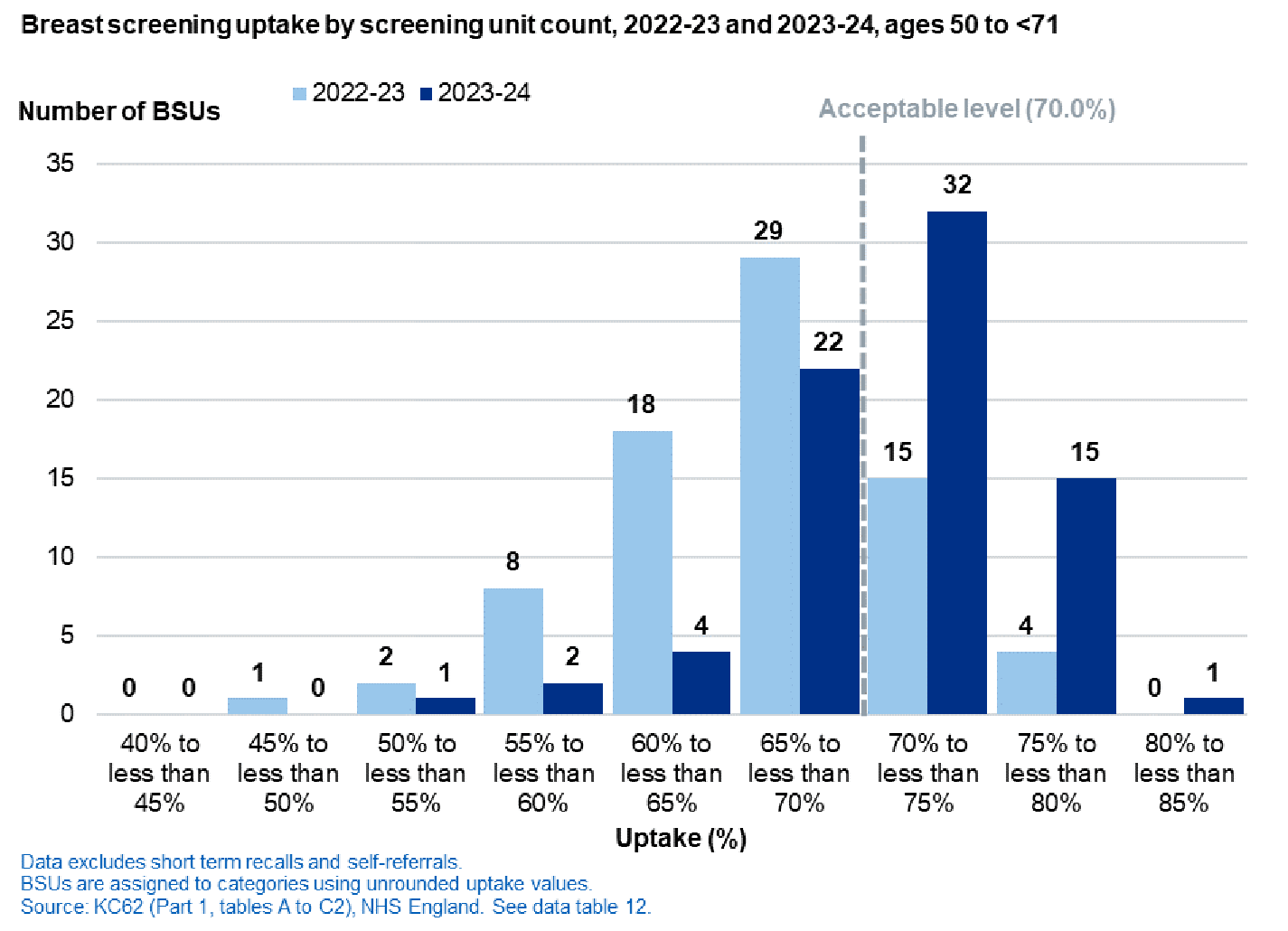
48 of 77 BSUs reached the acceptable level of 70%, 29 BSUs more than in 2022-23.
Uptake ranged from 54.6% to 80.7% at BSU level.
Uptake data by BSU can be explored further in the dashboard:
National (ages 50 to <71)
National uptake, by age, 2023-24
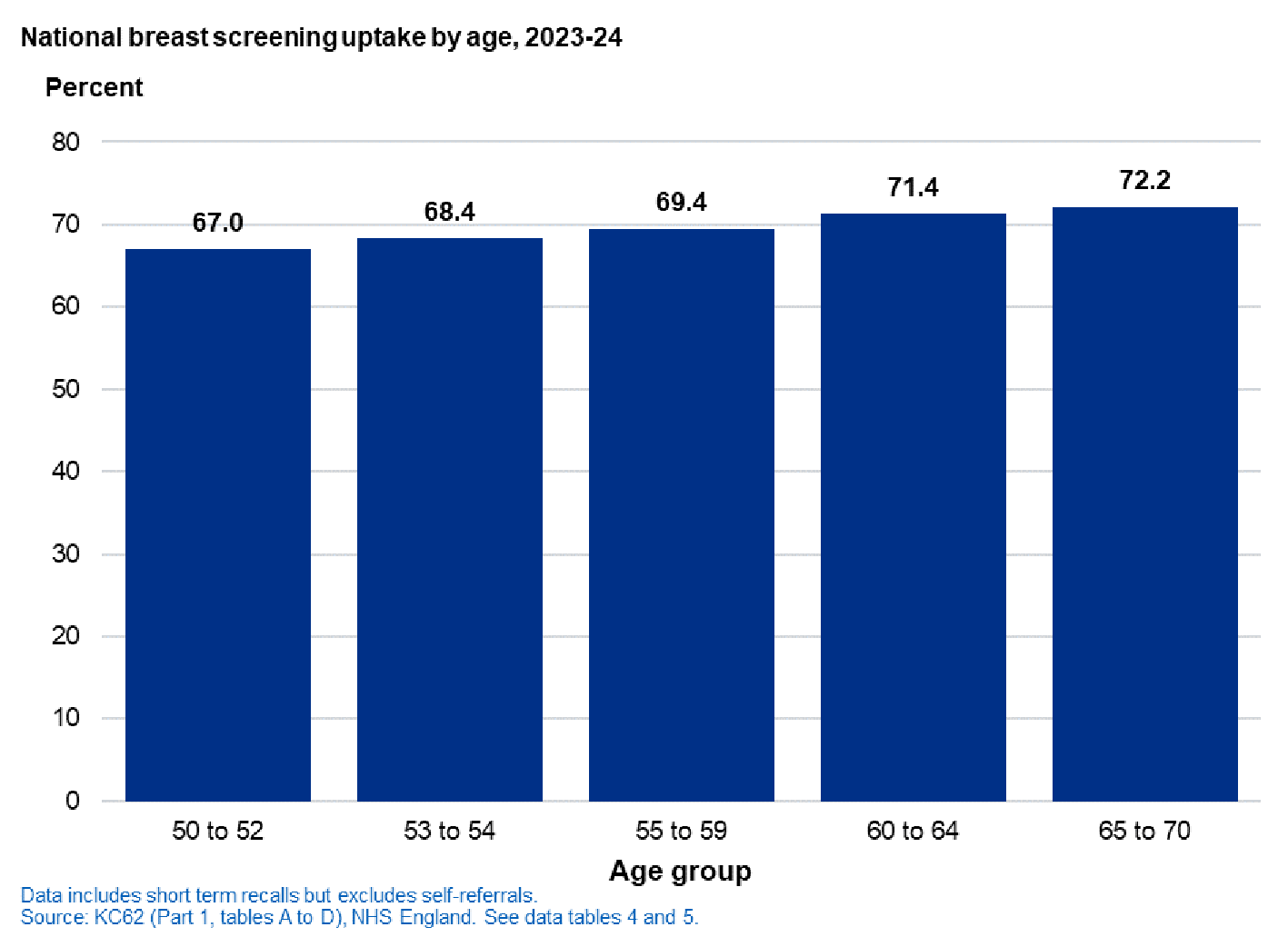
Uptake by women increased by age group, ranging from 67.0% (aged 50-52) to 72.2% (aged 65-70).
Uptake data by age can be explored further in the dashboard: http://bit.ly/breast_screen_annual_stats
Women are referred to an assessment clinic for further tests if a potential abnormality is detected at initial screening (see Appendix A).
Referrals for assessment are reported by two distinct screening types as the percentage of referrals is expected to vary according to type:
Prevalent screening refers to first invitations for routine screening and invitations to previous non-attendees.
Incident screening refers to routine invitations to previous attendees screened.
The programme aims to minimise the adverse effects of screening, such as anxiety and unnecessary investigations, and therefore the number of women this affects through referral for assessment.
Outcome of screening
National, referrals for assessment (ages 45 and over)
- In 2023-24, 6.1% of women attending for the first time (prevalent screening) were referred for assessment.
- 2.7% of women who had been previously screened (incident screening) were referred for assessment.
| 2022-23 | 2023-24 | ||||||||
| Referred for assessment(a) | Referred for assessment(a) | ||||||||
| Type of invitation/referral | Number screened | Number referred |
% | Number screened | Number referred |
% | |||
| Total | 2,176,856 | 72,858 | 3.3 | 1,951,323 | 68,664 | 3.5 | |||
| Prevalent screens | 259,402 | 16,189 | 6.2 | 322,169 | 20,295 | 6.3 | |||
| 1st invitation for routine screening | 203,121 | 12,522 | 6.2 | 249,492 | 15,296 | 6.1 | |||
| Routine invitation to previous non-attenders | 56,281 | 3,667 | 6.5 | 72,677 | 4,999 | 6.9 | |||
| Incident screens | 1,700,351 | 46,894 | 2.8 | 1,459,516 | 40,055 | 2.7 | |||
| Routine invitation to previous attenders (within five years) |
1,556,091 | 41,446 | 2.7 | 1,261,527 | 32,069 | 2.5 | |||
| Routine invitation to previous attenders (more than five years) |
144,260 | 5,448 | 3.8 | 197,989 | 7,986 | 4.0 | |||
| Other Short term recall(b) |
536 | 494 | 92.2 | 519 | 500 | 96.3 | |||
| Self/GP referral (no previous screen) | 32,655 | 2,228 | 6.8 | 34,449 | 2,372 | 6.9 | |||
| Self/GP referral (within 5 years) | 149,137 | 5,276 | 3.5 | 91,410 | 3,222 | 3.5 | |||
| Self/GP referral (>5 years) | 34,775 | 1,777 | 5.1 | 43,260 | 2,220 | 5.1 | |||
(a) Including women referred for cytology, core biopsy or open biopsy. See glossary for more information.
(b) Women invited under short term recall are invited to an assessment clinic rather than to routine screening.
(c) The technical definition recorded in the dataset is 'self / GP referral', however, the activity recorded under this definition is expected to only self-referrals as GPs do not make referrals to the screening programme.
Source: KC62 (Part 1, tables A to F2) NHS England – see data table 6.
All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
National, referrals for assessment by category (ages 45 and over), 2023-24
68,664 women were referred for assessment in 2023-24, down from 72,858 in 2022-23.
50.6% of women referred for assessment in 2023-24 underwent core biopsy and/or fine-needle aspiration cytology.
For further information see Appendix A.
1.2% of women referred for assessment were referred for open biopsy, up from 1.1% in 2022-23.
| Total referred for assessment(b) |
Referred for cytology and/or core biopsy(a) |
Referred for open biopsy |
||||
| Type of invitation/referral | Number | %(c) | Number | %(c) | ||
| Total | 68,664 | 34,720 | 50.6 | 810 | 1.2 | |
| Prevalent screens | 20,295 | 10,428 | 51.4 | 283 | 1.4 | |
| 1st invitation for routine screening | 15,296 | 7,716 | 50.4 | 217 | 1.4 | |
| Routine invitation to previous non-attenders | 4,999 | 2,712 | 54.3 | 66 | 1.3 | |
| Incident Screens | 40,055 | 20,004 | 49.9 | 445 | 1.1 | |
| Routine invitation to previous attenders (within five years) |
32,069 | 15,607 | 48.7 | 358 | 1.1 | |
| Routine invitation to previous attenders (more than five years) |
7,986 | 4,397 | 55.1 | 87 | 1.1 | |
| Other Short term recall |
500 | 78 | 15.6 | 3 | 0.6 | |
| Self/GP referral (no previous screen) | 2,372 | 1,145 | 48.3 | 26 | 1.1 | |
| Self/GP referral (within 5 years) | 3,222 | 1,748 | 54.3 | 28 | 0.9 | |
| Self/GP referral (>5 years) | 2,220 | 1,317 | 59.3 | 25 | 1.1 | |
(a) Including women referred for open biopsy after being referred for cytology and/or core biopsy.
(b) Including women referred for further imaging, or subsequently referred for cytology, core biopsy or open biopsy. See Appendix A for more information.
(c) The percentages for ‘Referred for cytology and/or core biopsy’ and ‘Referred for open biopsy’ are calculated using the total number of women referred for assessment as the denominator.
Source: KC62 (Parts 1 and 2, tables A to F2) NHS England – see data table 6.
National, short term recall outcomes (ages 45 and over), 2023-24
Amongst women who are referred for assessment following breast screening, a definitive diagnosis cannot be made in a very small number of cases. When this occurs women are recalled early for further assessment.
0.8% of women referred for assessment were recommended for short term recall.
| Assessment outcome - short term recall(a) |
|||
| Type of invitation / referral | Total referred for assessment(b) |
Number | %(c) |
| Total | 68,664 | 553 | 0.8 |
| Prevalent screens | 20,295 | 177 | 0.9 |
| 1st invitation for routine screening | 15,296 | 118 | 0.8 |
| Routine invitation to previous non-attenders | 4,999 | 59 | 1.2 |
| Incident screens | 40,055 | 287 | 0.7 |
| Routine invitation to previous attenders (within five years) |
32,069 | 213 | 0.7 |
| Routine invitation to previous attenders (more than five years) |
7,986 | 74 | 0.9 |
| Other Short term recall |
500 | 26 | 5.2 |
| Self/GP referral (no previous screen) | 2,372 | 27 | 1.1 |
| Self/GP referral (within 5 years) | 3,222 | 16 | 0.5 |
| Self/GP referral (>5 years) | 2,220 | 20 | 0.9 |
(a) Including all women whose final outcome was short term recall, whether after initial screen, assessment, cytology or biopsy (core or open).
(b) Including women subsequently referred for cytology, core biopsy or open biopsy. See Appendix A for more information.
(c) Note that the percentage of assessment outcomes that were ‘short term recalls’ is calculated using the total number of women referred for assessment as the denominator.
This differs from data tables 6, 7 and 7a where the denominator is the number of women screened.
Source: KC62 (Part 1, tables A to F2) NHS England – see data table 6.
Number of women with cancers detected
The number of women each year with cancer detected can be attributed to factors including changes to the number of women eligible for screening as a result of changes to the population.
i.e. as the population of women within the screening age range increases, the number of women eligible for screening will also increase. Therefore, the more women who are screened, the more potential cancers which will be detected. This is independent of the rate of detection
Rate of cancer detection
The cancer detection rate may be influenced by the following factors:
- The age distribution of women screened in any one year, as the incidence of breast cancer increases with age6.
- The expansion of the screening programme to broader, largely older, age groups in the last ten years.
- Targeted awareness campaigns.
- The introduction of digital mammography in 2008 which was fully implemented by 2016.
National (ages 45 and over)
National detection, by age, 2022-23 and 2023-24
- In 2023-24, 16,677 women had cancers detected by the programme, a rate of 8.5 cases per 1,000 women screened (a decrease from a rate of 8.7 in 2022-23).
- Amongst the core programme (50-<71 years), the detection rate was 8.1 per 1,000 in 2023-24 (a decrease from a rate of 8.2 in 2022-23).
| 2022-23 | 2023-24 | ||||||
| Cancers detected | Cancers detected | ||||||
| Age group | Number screened | Women with cancer | Rate per 1,000 women screened | Number screened | Women with cancer | Rate per 1,000 women screened | |
| 45 and over | 2,176,856 | 18,942 | 8.7 | 1,951,323 | 16,677 | 8.5 | |
| 45 - 49 | 23,151 | 163 | 7.0 | 29,158 | 192 | 6.6 | |
| 50 - 70 | 2,031,091 | 16,662 | 8.2 | 1,838,932 | 14,970 | 8.1 | |
| 71 - 74 | 59,918 | 922 | 15.4 | 39,645 | 621 | 15.7 | |
| 75 and over | 62,696 | 1,195 | 19.1 | 43,588 | 894 | 20.5 | |
Source: KC62 (Parts 1 and 3, table T) NHS England - see data table 9a.
National detection, by age, 2013-14 to 2023-24
- The incidence of breast cancer detected through screening increases with age.
- In 2023-24, detection rates were lowest for women aged 45-49 (6.6 per 1,000) and highest for women aged 71 or over (18.2 per 1,000).
- There was a decrease in detection rates for most age groups in 2023-24, but an increase for women aged 50-54 and women aged 71 or over.
- All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
National detection, by age (45 and over), 2023-24
- In prevalent screens, the rate of women aged 45 and over with cancer detected was 8.5 per 1,000 women screened. In incident screens, the rate was 7.9 per 1,000.
- The cancer detection rate was highest in short term recalls (36.6 per 1,000 women).
- It would be expected that the detection rate is highest for short term recalls as in these cases women have been referred for assessment following an abnormal mammogram but following further tests a definitive diagnosis could not be made. Short term recalls should be an exceptional outcome of assessment and will only occasionally occur.
| Rate per 1,000 women screened | ||||||||
| Type of invitation / referral | 45+ | 50-70 | 45-49 | 50-54 | 55-59 | 60-64 | 65-70 | 71+ |
| Total | 8.5 | 8.1 | 6.6 | 6.8 | 6.9 | 8.5 | 10.6 | 18.2 |
| Prevalent screens | 8.5 | 8.7 | 6.6 | 7.8 | 10.2 | 15.6 | 19.7 | 15.4* |
| 1st invitation for routine screening | 7.7 | 7.8 | 6.6 | 7.7 | 8.3 | 12.0 | 13.3 | 15.4* |
| Routine invitation to previous non-attenders | 11.2 | 11.2 | - | 8.6 | 10.7 | 17.2 | 24.0 | 15.9* |
| Incident screens | 7.9 | 7.8 | - | 5.4 | 6.5 | 8.1 | 10.2 | 12.6 |
| Routine invitation to previous attenders (within five years) |
7.2 | 7.2 | - | 5.3 | 6.2 | 7.3 | 9.3 | 11.7 |
| Routine invitation to previous attenders (more than five years) |
11.9 | 11.9 | - | 7.2 | 8.7 | 12.5 | 15.7 | 17.6* |
| Other Short term recall |
36.6* | 31.7* | - | 11.4* | 17.2* | 69.8* | 52.6* | 88.9* |
| Self/GP referral (no previous screen) | 11.7 | 10.9 | 10.4* | 9.3 | 12.3 | 16.1 | 15.7* | 21.1 |
| Self/GP referral (within 5 years) | 12.9 | 9.8 | - | 6.5 | 7.9 | 10.5 | 15.3 | 15.8 |
| Self/GP referral (>5 years) | 20.0 | 14.7 | - | 5.8* | 11.2 | 16.0 | 20.4 | 23.5 |
- = Zero.
* Rate based on fewer than 2,000 women screened.
Source: KC62, Parts 1 and 3 (tables A to F2, T) NHS England - see data tables 8 and 9a.
National (ages 45 and over)
The overarching aim of breast screening is to reduce mortality by finding breast cancer at an early stage when the changes in the breast are often too small to detect by hand.
Cancers are reported in two main categories, non-invasive and invasive. Invasive cancers are then reported by two further sub categories.
Non-invasive or micro-invasive cancer is one which demonstrates no or only very slight (<1mm) invasion into adjacent tissues.
Invasive cancer is one which has spread beyond the layer of tissue in which it has developed and is growing into surrounding, healthy tissues.
- Small invasive cancers (size of less than 15mm)
- Invasive cancers (size of 15mm or greater)
National detection, by cancer type or size, 2013-14 to 2023-24
In 2023-24, detection rates were highest for invasive and small invasive cancers (3.2 per 1,000 women) and lowest for non-invasive or micro-invasive cancers (1.8 per 1,000 women).
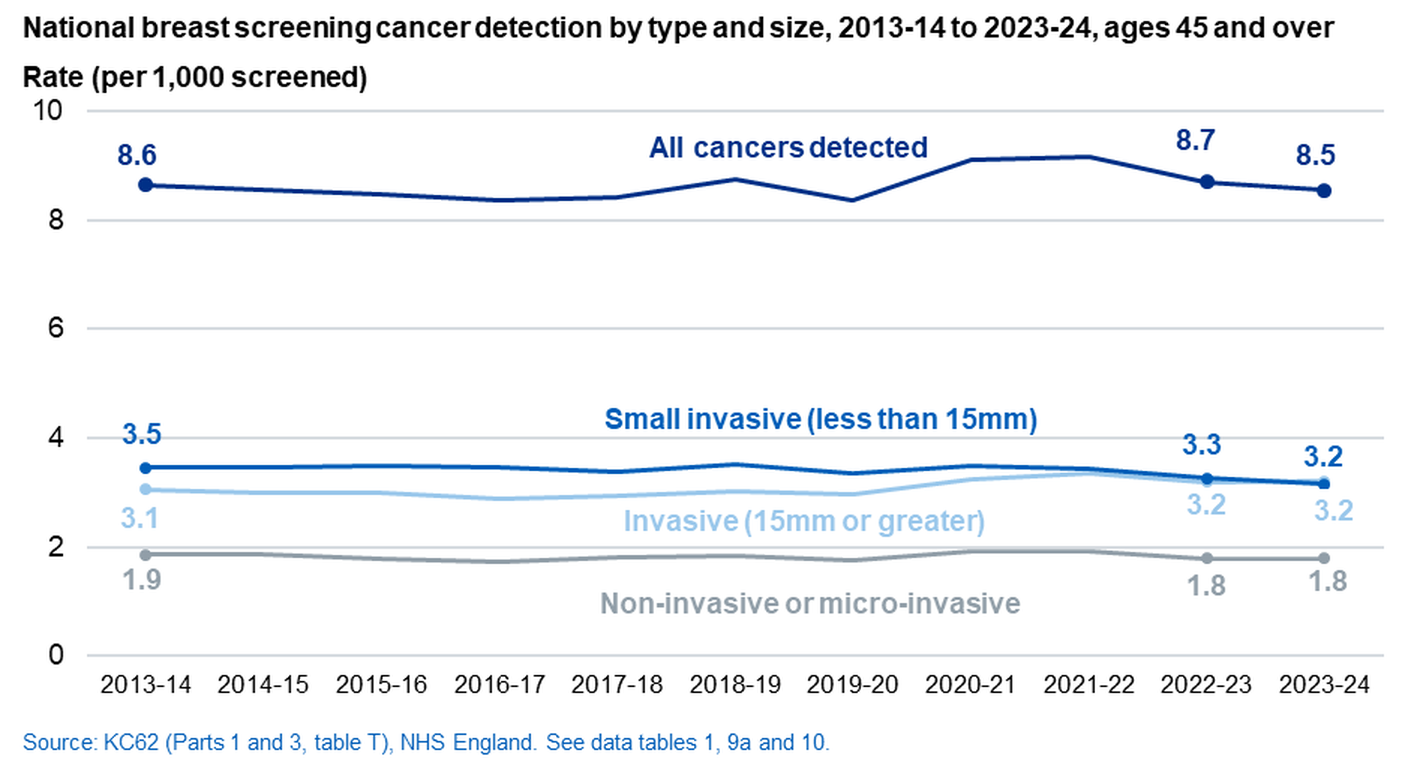
The breakdowns in the chart above exclude the sub-categories ‘Invasive status not known’ (4 in 2023-24) and ‘Invasive – size not known’ (765 in 2023-24). See data tables 9a and 10 for full data.
All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
National (ages 45 and over)
National detection, by type / size of cancer, 2022-23 and 2023-24
| 2022-23 | 2023-24 | ||||
| Type / size of cancer | Total with cancer |
% | Total with cancer | % | |
| Total | 18,942 | 100.0 | 16,677 | 100.0 | |
| Invasive status not known | 12 | 0.1 | 4 | 0.0 | |
| Non-invasive or micro-invasive | 3,900 | 20.6 | 3,482 | 20.9 | |
| Total invasive | 15,030 | 79.3 | 13,191 | 79.1 | |
| Invasive – small (<15mm) | 7,105 | 37.5 | 6,161 | 36.9 | |
| Invasive (>=15mm) | 6,950 | 36.7 | 6,265 | 37.6 | |
| Size not known | 975 | 5.1 | 765 | 4.6 | |
NB: The sum of components may not equal totals due to rounding.
Source: KC62 (Part 3, table T) NHS England - see data table 10.
All breast screening services were impacted by disruption from the COVID-19 pandemic between 2020-21 and 2022-23 - see COVID impact summary for more details.
- In 2023-24, 20.9% of women aged 45 and over with cancer detected had non-invasive or micro-invasive cancers.
- 79.1% had invasive cancers of any size.
- Small invasive cancers accounted for 46.7% of all invasive cancers, and 36.9% of all cancers.
National (ages 50-<71), 2023-24
- At the prevalent screen, 26.6% of all cancers detected were non-invasive cancers and 30.4% were small invasive cancers.
- At the incident screen, 20.4% of all cancers detected were non-invasive cancers and 39.4% were small invasive cancers.
| Total with cancer |
Non-invasive or micro-invasive cancer |
Invasive cancer | ||||
| Total invasive(a) |
Small invasive (<15mm) |
Invasive (>=15mm) |
||||
| Type of invitation/referral | % of total with cancer |
% of total with cancer |
% of total with cancer |
% of total with cancer |
||
| Total | 14,970 | 21.4 | 78.6 | 37.4 | 36.8 | |
| Prevalent screens | 2,538 | 26.6 | 73.3 | 30.4 | 38.4 | |
| 1st invitation for routine screening | 1,724 | 28.2 | 71.8 | 30.9 | 36.9 | |
| Routine invitation to previous non-attenders | 814 | 23.3 | 76.5 | 29.4 | 41.5 | |
| Incident screens | 11,402 | 20.4 | 79.6 | 39.4 | 36.0 | |
| Routine invitation to previous attenders (within five years) |
9,058 | 20.6 | 79.4 | 40.3 | 35.3 | |
| Routine invitation to previous attenders (more than five years) |
2,344 | 19.7 | 80.3 | 35.8 | 38.5 | |
| Other Short term recall |
15 | 40.0 | 60.0 | 46.7 | 13.3 | |
| Self/GP referral (no previous screen) | 347 | 20.5 | 79.5 | 30.5 | 43.5 | |
| Self/GP referral (within 5 years) | 420 | 18.8 | 81.2 | 35.5 | 40.2 | |
| Self/GP referral (>5 years) | 248 | 16.9 | 83.1 | 32.3 | 43.1 | |
(a) Includes some invasive cancers of unknown size.
Source: KC62 (Part 3, tables A to F2, T) NHS England - see data tables 8, 10 and 10a.
National (ages 50-<71), 2023-24
- In 2023-24, small cancers (less than 15mm in diameter) accounted for 47.6% of those with invasive cancer.
- In prevalent screens this figure is 41.4%.
- In incident screens this figure is 49.5%.
| Total invasive |
Small invasive (<15mm) |
Invasive (>=15mm) |
Invasive (size unknown) |
|
| Type of invitation/referral | % of total invasive |
% of total invasive |
% of total invasive |
|
| Total | 11,769 | 47.6 | 46.8 | 5.6 |
| Prevalent screens | 1,861 | 41.4 | 52.4 | 6.2 |
| 1st invitation for routine screening | 1,238 | 43.0 | 51.5 | 5.6 |
| Routine invitation to previous non-attenders | 623 | 38.4 | 54.3 | 7.4 |
| Incident screens | 9,076 | 49.5 | 45.2 | 5.3 |
| Routine invitation to previous attenders (within five years) |
7,193 | 50.7 | 44.5 | 4.8 |
| Routine invitation to previous attenders (more than five years) |
1,883 | 44.6 | 48.0 | 7.4 |
| Other Short term recall |
9 | 77.8 | 22.2 | 0.0 |
| Self/GP referral (no previous screen) | 276 | 38.4 | 54.7 | 6.9 |
| Self/GP referral (within 5 years) | 341 | 43.7 | 49.6 | 6.7 |
| Self/GP referral (>5 years) | 206 | 38.8 | 51.9 | 9.2 |
Source: KC62 (Part 3, Tables A to F2, T) NHS England - see Data Tables 8, 10 and 10a.
Cancer detection rates in other UK countries
Women at higher risk are those who have been assessed by a specialist in genetics or oncology as being at greater risk of developing breast cancer than women in the general population7. Women at very high risk7 are eligible for screening in the NHS BSP and are screened as part of the programme.
Women at very high risk of developing breast cancer are offered breast screening at an earlier age and at different frequencies to women in the general population7.
In addition to a mammogram, these women may also be screened using a magnetic resonance imaging (MRI) scanner; a large tube surrounded by a strong magnetic field.
Since 2017-18, high-risk data in this section has been collected using a new and more comprehensive collection system.
2020-21 was the first year that the new breakdowns were available for use in the annual report.
By risk category
England, 2023-24
A total of 11,660 women at very high risk of developing breast cancer were screened in 2023-24.
Of those screened, the majority were in the BRCA 1 and BRCA 2 risk categories.

Cancer detection rates, by risk category
Cancer detection rates for the largest risk categories are presented in the table below
| Rate per 1,000 women screened | ||
| High risk category | Total Cancers(1) | Invasive Cancers(2) |
| All risk categories | 19.5 | 15.5 |
| Genetic / Familial Risk BRCA 1 |
20.5 | 16.6 |
| BRCA 2 | 22.4 | 18.7 |
| Not tested | 13.1 | 8.4 |
| Radiotherapy (Irradiated <36) |
19.9 | 14.4 |
(1)For comparison, the national rate for cancers detected per 1,000 women screened in 2023-24, for women aged 50-<71 is 8.1
(2)For comparison, the national rate for invasive cancers detected per 1,000 women screened in 2023-24, for women aged 50-<71 is 6.4
BRCA1 = Breast cancer gene 1, BRCA 2 = Breast cancer gene 2
Source: KC62 (Table U3) NHS England - see data table 16.
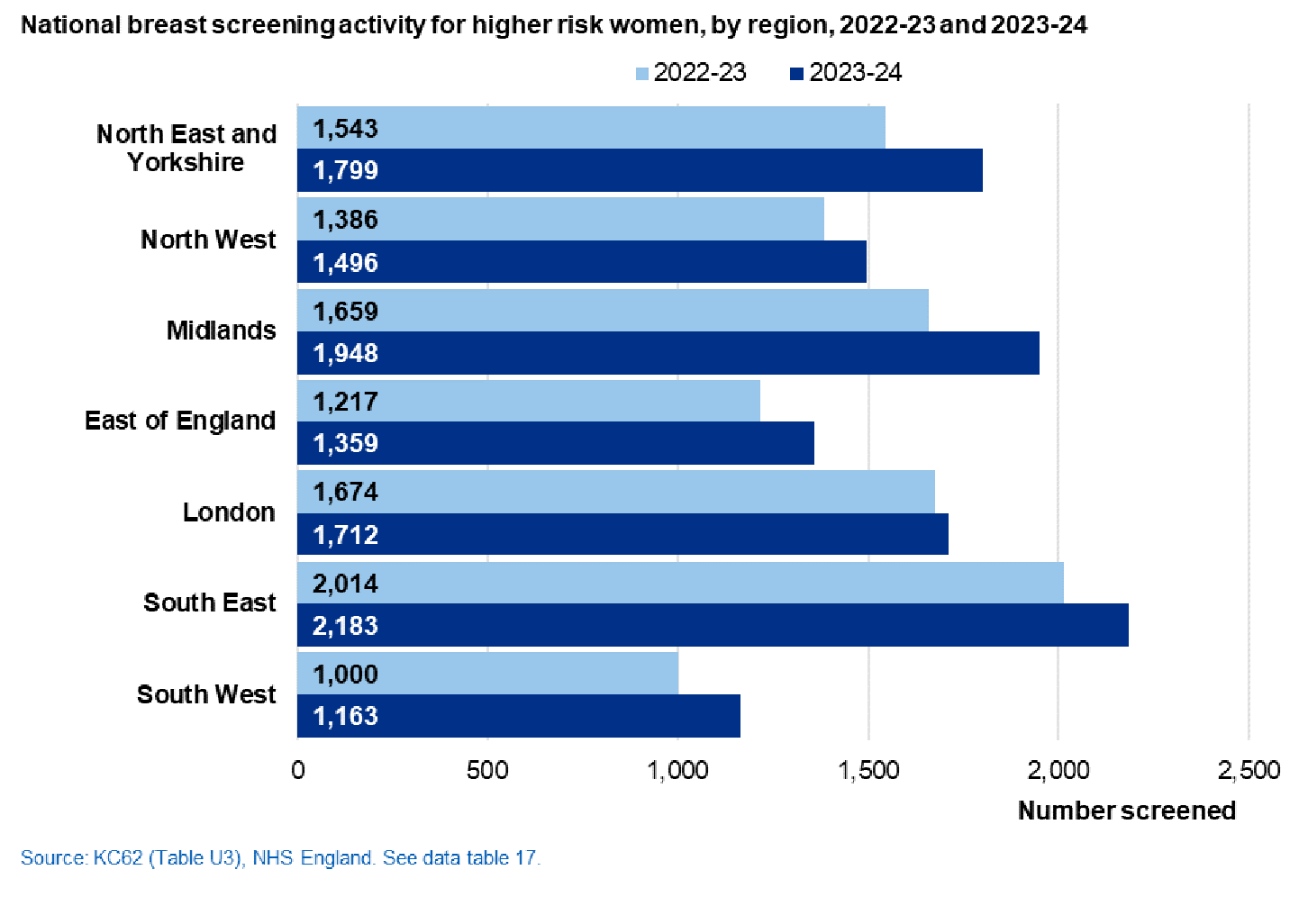
By region
England, 2023-24
The South East region had the greatest number of women screened who were at higher risk of developing breast cancer.
Glossary
Assessment ‘Further diagnostic tests’ that do not include ‘repeat examinations’9
Benign Not cancer. Not malignant. A benign tumour does not invade surrounding tissue or spread to other parts of the body10 .
Bilateral mastectomy Surgical removal of both breasts.
Biopsy A medical procedure that involves taking a small sample of tissue so that it can be examined under a microscope10.
Breast screening unit (BSU) In 2023-24 there were 77 breast screening units (BSU) in England which deliver local screening programmes.
Coverage The percentage of women in the population who are eligible for screening at a particular point in time (31 March 2024 in this report), who have had a test with a recorded result at least once within the screening round, i.e. in the previous three years. Currently coverage is best assessed using the 53-70 age group.
Cytology The medical and scientific study of cells. A branch of pathology, the medical specialty that deals with making diagnoses of diseases and conditions through the examination of tissue samples from the body10.
Eligibility Women are eligible for screening when in the screening age range, unless they are ceased due to the following: women who have had bilateral mastectomies. In order for an invitation to be sent, an individual must be registered at a GP practice. Note: Women who are excluded due to a best interests decision or who request to opt-out from screening will no longer receive invitations for screening but are included in the eligible population.
Fine-needle aspiration cytology Where samples of breast cells or fluid are drawn off through a very fine needle.
Incident Screening Screening of women who have been previously screened within the NHS Breast Screening Programme. In this statistical bulletin, incident screening figures relate only to routine invitations to previous attenders last screened within five years.
Invasive cancer Cancer which has spread beyond the layer of tissue in which it developed and is growing into surrounding, healthy tissues.
Magnetic resonance imaging (MRI) A type of scan that uses strong magnetic fields and radio waves to produce detailed images of the inside of the body11
Mammogram X-rays of each breast. Mammography can detect small changes in breast tissue which may indicate cancers which are too small to be felt either by the woman herself or by a doctor12.
Mastectomy Surgical removal of the whole breast.
Non- or micro-invasive cancer A cancer which demonstrates no or only very slight invasion into adjacent tissues by malignant cells of a carcinoma in situ.
Open biopsy A minor operation to take one or more samples of tissue under general anaesthetic. Also known as excision or surgical biopsy.
Prevalent screening Screening of women never previously screened within the NHS Breast Screening Programme. In this statistical bulletin, prevalent screening figures relate to first invitations for routine screening and routine invitations to previous non-attendees.
Repeat examinations Repeat examinations include both those images repeated with the same view while the woman is still present in the unit, and those occasions when a woman is required to attend a second time to have a film repeated (same view) because of a technical inadequacy13.
Short term recall A second invitation to attend an assessment clinic at less than the routine (three year) screening interval13 .
Uptake The percentage of eligible women invited for screening in the year, who were screened adequately within six months of invitation14.
1. See glossary for definition of eligibility.
2. Programme screening standards valid for data collected from 1 April 2017 https://www.gov.uk/government/publications/breast-screening-consolidated-programme-standards
3. https://www.gov.uk/government/publications/breast-screening-consolidated-programme-standards
4. https://www.gov.uk/government/publications/opting-out-of-breast-screening
5. Short term recall is a non-routine invitation at less than a standard screening interval following assessment
6. NHS Cancer Screening Programmes: http://www.nhs.uk/conditions/breast-cancer-screening/Pages/Introduction.aspx
7. See https://www.gov.uk/government/publications/nhs-breast-screening-high-risk-women and https://www.gov.uk/government/publications/breast-screening-higher-risk-women-surveillance-protocols
9. ‘Breast screening: consolidated programme standards’ https://www.gov.uk/government/publications/breast-screening-consolidated-programme-standards
10. National Cancer Institute: https://www.cancer.gov/publications/dictionaries/cancer-terms
11. NHS Choices - http://www.nhs.uk/Conditions/MRI-scan/Pages/Introduction.aspx
12. NHS Breast Screening Programme: http://www.nhs.uk/conditions/breast-cancer-screening/Pages/Introduction.aspx
13. ‘Guidance for breast screening mammographers ’, September 2020, NHS Breast Screening Programme https://www.gov.uk/government/publications/breast-screening-quality-assurance-for-mammography-and-radiography
14. ‘Clinical guidance for breast cancer screening assessment ’, November 2016, NHS Breast Screening Programme https://www.gov.uk/government/publications/breast-screening-clinical-guidelines-for-screening-management
Last edited: 18 February 2025 9:31 am